
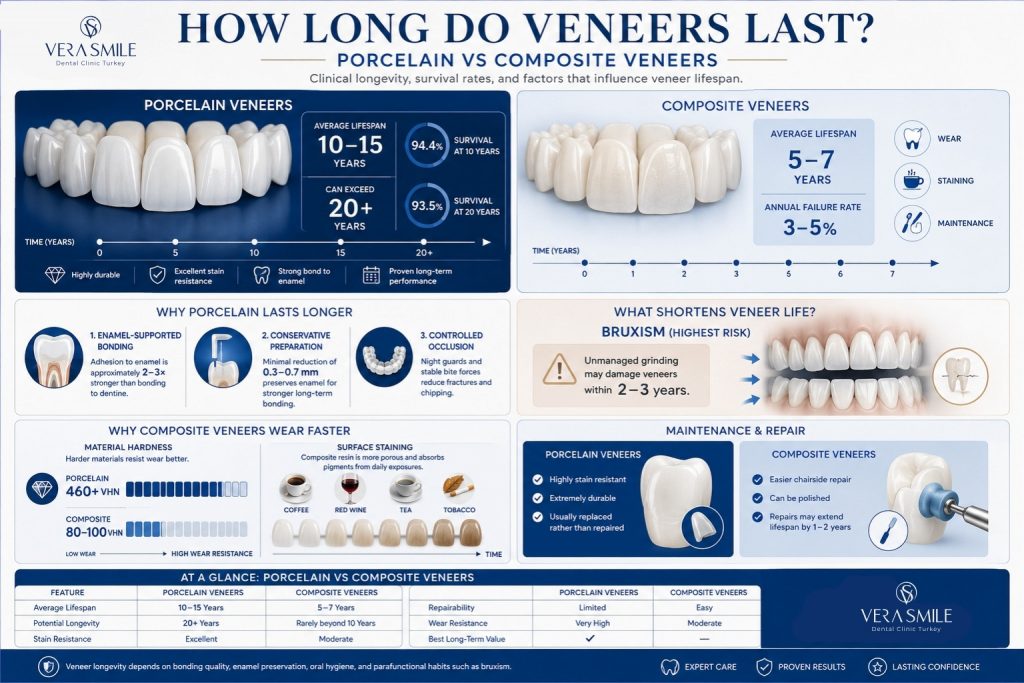
Porcelain veneers last 10 to 15 years on average, lithium disilicate (E.max) veneers last 12 to 20 years, and composite veneers last 5 to 7 years when fitted correctly and maintained well. Lifespan is shaped by four variables: the ceramic or resin used, the bonding protocol, the patient’s oral environment, and the precision of the underlying tooth preparation. Long-term prospective studies report a 10-year survival rate above 93% for porcelain veneers and close to 83% at 20 years under controlled conditions.
Composite veneers wear and discolour faster because the resin matrix is softer and more porous than ceramic. End-of-life veneers are replaced, not repaired. Dental veneers in every material class follow the same principle: material and technique set the ceiling, and daily habits decide where the veneer lands beneath it. At Vera Smile, material selection follows the same survival evidence, with enamel coverage, occlusal load, and aesthetic demands deciding the ceramic, and patients with unmanaged bruxism or insufficient enamel redirected to alternatives first.
How Does Veneer Lifespan Compare by Material?
Dental veneers last between 5 and 20 years on average, depending on material. Porcelain sits around 10 to 15 years, lithium disilicate (E.max) around 12 to 20 years, and composite around 5 to 7 years in published clinical reviews.
| Veneer material | Average lifespan | 5-year survival | 10-year survival | Most common failure mode |
|---|---|---|---|---|
| Porcelain (feldspathic) | 10–15 years | 95% | 93% | Marginal fracture, debonding |
| Lithium disilicate (E.max) | 12–20 years | 95–98% | 94% | Bulk fracture under heavy load |
| Composite (direct) | 5–7 years | 85% | 50–65% | Wear, staining, chipping |
Survival values are pooled from prospective veneer studies and Cochrane-aligned reviews. Real-world outcomes vary with operator skill, patient bite forces, and follow-up adherence.
How Long Do Porcelain Veneers Last?
Porcelain veneers last 10 to 15 years on average, with well-documented cases extending beyond 20 years. A long-term prospective study of 318 feldspathic veneers reported a cumulative survival rate of 94.4% at 10 years and 93.5% at 20 years.
Three clinical conditions push porcelain veneer survival into the upper range. The first is enamel-supported bonding: adhesion to enamel is roughly two to three times stronger than to dentine, so veneers seated on enamel-rich margins debond far less often. The second is conservative preparation depth, since removal limited to 0.3 to 0.7 mm preserves the enamel layer that anchors the adhesive interface. The third is controlled occlusion, because patients without parafunction, or those who wear a night guard, record fewer fractures and chips over years of function.
Bruxism remains the strongest negative predictor. Unmanaged grinding can compromise a porcelain veneer within 2 to 3 years.
How Long Do Composite Veneers Last?
Composite veneers last 5 to 7 years on average, with annual failure rates between 3% and 5% reported in pooled clinical reviews of anterior composite restorations. Composite is a polymer-based material, so it wears, stains, and loses surface gloss faster than glass-ceramic alternatives.
Two factors explain the shorter timeline. Resin matrix wear is the first: composite hardness sits around 80 to 100 VHN, well below porcelain at 460+ VHN, so masticatory wear accumulates more visibly each year. Surface staining is the second, because the resin is more porous than ceramic and absorbs pigments from coffee, tea, red wine, and tobacco within the first 24 months of service.
Direct composite veneers can be polished or partially repaired chairside, which extends service life by 1 to 2 years compared with replacement-only ceramics. Indirect (lab-fabricated) composite veneers perform slightly better than direct composite but still fall short of porcelain in long-term studies.
How Long Do Lithium Disilicate (E.max) Veneers Last?
Lithium disilicate veneers, often marketed as E.max, last 12 to 20 years on average, with 5-year survival rates of 95% or higher in multiple clinical investigations. The material delivers a higher flexural strength (around 360 to 400 MPa) than feldspathic porcelain (around 60 to 90 MPa).
That mechanical advantage translates into lower fracture risk under masticatory load, thinner preparation tolerances that preserve more natural tooth structure, and better fatigue resistance in long-term cyclic-loading studies. In practical terms, the denser glass-ceramic structure absorbs the daily forces that cause bulk fractures in weaker ceramics, while permitting restorations thin enough to keep the preparation inside enamel.
Lithium disilicate veneers still depend on enamel-bonded margins for adhesive longevity. When more than half of the margin sits in dentine, survival rates drop in line with feldspathic porcelain. Porcelain veneers remain the closest clinical alternative when enamel coverage is sufficient and bite forces are moderate.
What Factors Affect How Long Veneers Last?
Several clinical and patient-side variables drive veneer lifespan. The list below summarises the most evidence-supported factors.
- Veneer material: Porcelain and lithium disilicate outlast composite because the ceramic matrix resists wear, staining, and fatigue better than resin.
- Enamel coverage at margins: Veneer survival improves when at least 50% of the prepared surface remains in enamel, since enamel-to-porcelain adhesion is stronger and more durable than dentine bonding.
- Tooth preparation depth: Minimally invasive preparation (0.3 to 0.7 mm) preserves enamel and lowers debonding risk over time.
- Occlusion and bruxism: Heavy grinding roughly doubles ceramic fracture risk; unmanaged bruxers may experience failure within 2 to 3 years.
- Oral hygiene: Plaque accumulation at veneer margins drives recurrent decay, the leading cause of veneer loss after year 10.
- Patient habits: Nail biting, ice chewing, and using teeth as tools introduce point loads that exceed ceramic flexural strength.
- Diet and oral pH: Frequent exposure to acidic foods and drinks erodes the bonded enamel substrate and weakens the cement line.
- Clinician experience: Operator skill is a documented variable in veneer survival, with better marginal seal and isolation linked to fewer reinterventions.
- Maintenance compliance: Routine professional cleanings and bite checks catch early problems before they become structural failures.
These variables compound, so two patients with identical veneers can record very different outcomes a decade later.
What Are the Most Common Reasons Veneers Fail?
Most veneer failures fall into a small number of repeatable failure modes. Knowing them helps patients spot warning signs early.
- Debonding: Loss of the adhesive bond between veneer and tooth, more common when preparation extends into dentine or when isolation was compromised during cementation.
- Bulk fracture: Cracks or pieces breaking off the ceramic, often linked to bruxism, occlusal interference, or trauma.
- Chipping at the incisal edge: Small fractures along the biting edge caused by edge-to-edge contacts or oral habits.
- Marginal staining: Dark line at the cement interface from microleakage, polish loss, or smoking.
- Recurrent caries: Decay forming at the veneer margin, almost always tied to declining home hygiene over years.
- Gum recession: Soft-tissue retraction that exposes the veneer margin and breaks the biological and optical seal.
- Pulpal complications: Sensitivity or pulp inflammation when preparation has approached the pulp chamber.
- Colour mismatch over time: Composite veneers in particular fall out of shade match as natural teeth and the resin age at different rates.
Most failures appear at the margin first. Margin condition is the single best clinical predictor of remaining service life, which is why the American Dental Association consumer guidance on veneers recommends regular professional checks of the veneer-tooth interface.
How Can Patients Make Veneers Last Longer?
Patient behaviour controls a large share of veneer lifespan after cementation. The actions below have measurable effects in clinical follow-up data.
- Maintain rigorous oral hygiene: Twice-daily brushing with a low-abrasive paste and daily interdental cleaning keeps plaque off the veneer margins, the most common decay site.
- Wear a night guard if bruxing: A custom-fitted occlusal guard reduces nocturnal loading on porcelain veneers and is the single most effective protective measure for grinders.
- Attend professional cleanings every six months: Hygiene visits remove biofilm where home tools cannot reach and let the dentist verify margin integrity early.
- Avoid biting hard objects: Ice, hard candy, pens, and fingernails introduce point loads above the flexural strength of most veneer ceramics.
- Limit highly pigmented and acidic drinks: Coffee, red wine, and acidic sports drinks accelerate marginal staining and erode the enamel that supports the bond.
- Quit smoking: Tobacco discolours luting cement at the margin and elevates periodontal recession around veneers.
- Use a soft-bristled brush: Hard bristles abrade porcelain glaze over years of use and dull reflectivity.
- Follow occlusal recommendations: Compliance with bite adjustments or guard use directly extends restoration life.
Daily habits, applied consistently, often add several years of clinical service to a well-placed veneer.
When Should Veneers Be Replaced?
Veneers should be replaced when clinical or radiographic findings indicate structural, biological, or aesthetic failure. Replacement is the standard endpoint because bonded ceramics cannot be reliably re-cemented after debond contamination.
- Visible cracks or chips: A fracture line across the veneer indicates structural compromise and warrants replacement, not polishing.
- Marginal leakage: A dark line at the gumline signals microleakage, which precedes recurrent decay.
- Recurrent decay at the margin: Cavities seen on bitewing X-rays around the veneer edge require veneer removal, caries control, and refabrication.
- Loss of adhesion: A loose veneer cannot be rebonded predictably because the cement layer and bonding surface are contaminated.
- Significant gum recession: Recession of 1.5 mm or more often exposes the veneer margin and disrupts the optical and biological seal.
- Severe colour change: Composite veneers may turn dull, yellow, or mismatched as the resin ages and the adjacent enamel changes.
- Bite changes affecting fit: Orthodontic relapse, tooth movement, or new restorations elsewhere can shift veneer contact points and require new fabrication.
A six-month dental review remains the most reliable way to catch these signs before they progress.
Do Digital Workflows Like Digital Smile Design Improve Veneer Longevity?
Yes. Digital workflows extend veneer lifespan indirectly by improving fit, occlusal precision, and margin accuracy. They do not change the underlying ceramic, but they reduce the technique-sensitive variables that drive most early failures.
Three digital tools matter clinically. Digital Smile Design (DSD) is a planning protocol that aligns aesthetic design with functional occlusion before any tooth is prepared, which lowers the rate of remakes for fit or aesthetic mismatch. 3D intraoral scanning replaces conventional impressions and produces a digital model with marginal accuracy in the 20 to 50 micron range, supporting a tighter cement seal. CAD/CAM dentistry then mills or presses restorations from those digitally designed files, reducing manual variability and improving the consistency of fit at the margin.
These workflows do not make veneers permanent. They raise the floor of expected outcomes, especially for full-mouth aesthetic cases where occlusal harmony has a strong influence on long-term survival.
Can Veneers Last a Lifetime?
No. Veneers are restorative, not permanent. Every veneer reaches an end-of-life point because the bonding cement, the ceramic, and the underlying enamel all change over decades of clinical service.
“Lifetime veneers” is a marketing label, not a clinical category. Some patients keep porcelain or lithium disilicate veneers for 20 to 25 years, but the median survival reported in long-term literature does not exceed 20 years, and individual veneers within the same arch may fail at different intervals. Planning for one or two replacement cycles across a patient’s lifetime is the realistic clinical assumption.
How Does Vera Smile Select Veneer Materials?
Vera Smile selects veneer material case by case, using three clinical variables: enamel coverage at the margins, occlusal load, and the translucency demands of the smile design. Material selection at the clinic follows the survival evidence, not the price list or the patient’s first request.
- Lithium disilicate (E.max): Considered where bite forces are moderate to high or where preparations must stay thin, because its 360 to 400 MPa flexural strength tolerates load while keeping the preparation inside enamel.
- Feldspathic porcelain: Suited to anterior cases where translucency demands are high, enamel coverage is near-complete, and occlusion is controlled.
- Composite: Positioned as a transitional or budget option, with the 5 to 7 year lifespan expectation stated in the written treatment plan rather than implied verbally.
One common industry practice Vera Smile disagrees with is the aggressive “instant smile makeover” preparation that cuts deep into dentine to speed up full-set cases. In Vera Smile Dental Clinic this approach is refused, because margins seated in dentine roughly halve adhesive longevity and convert a 15-year restoration into a 7-year one. The same reasoning applies to veneering teeth that only need whitening: when bleaching can achieve the shade goal, the clinic recommends bleaching and declines to remove healthy enamel.
What Does the Vera Smile Bonding Protocol Include
The bonding sequence below is the standard cementation protocol applied to ceramic veneers at Vera Smile, aligned with Slow Dentistry Global Network requirements.
| Protocol stage | What is done | Why it matters for lifespan |
|---|---|---|
| Isolation | Rubber dam placed before any adhesive step | Saliva contamination is the leading cause of early debonding |
| Ceramic conditioning | Hydrofluoric acid etch followed by silane application | Creates the chemical bond between resin cement and glass-ceramic |
| Enamel conditioning | Selective phosphoric acid etch of the prepared surface | Enamel adhesion is two to three times stronger than dentine adhesion |
| Cementation | Light-cured resin cement with controlled excess removal | A sealed, void-free margin delays microleakage and staining |
| Occlusal verification | Bite check, adjustment, and night-guard decision before discharge | Uncontrolled load is the strongest predictor of ceramic fracture |
Each stage is time-controlled rather than volume-controlled, which is the practical difference between a protocol designed for longevity and one designed for daily patient throughput.
Who Is Not a Candidate for Veneers at Vera Smile?
Vera Smile declines or redirects veneer requests when the clinical findings predict early failure, because placing a veneer that the evidence says will fail within a few years is not treatment. The decline criteria used at the clinic are listed below.
- Unmanaged bruxism: Patients who grind and decline night-guard use are not veneered, since unmanaged grinding can fracture ceramic within 2 to 3 years.
- Insufficient enamel at the margins: When more than half of the bonding surface would sit in dentine, the clinic recommends a full-coverage crown instead, because dentine-seated veneers debond at significantly higher rates.
- Active gum disease or untreated decay: Periodontal treatment and caries control are completed first; veneering over inflamed tissue guarantees marginal problems.
- Severe malocclusion: Bites that would load veneers edge-to-edge are referred for orthodontic correction before any ceramic is planned.
- Whitening-only goals: Patients whose only complaint is shade are offered professional bleaching first, because cutting healthy enamel for a colour change is irreversible and unnecessary.
A case from clinic records illustrates the policy: a [DATA NEEDED: anonymised real case confirmed by the medical team; structure: patient profile, presenting request, clinical finding at assessment, revised treatment plan, outcome at follow-up].
Declining a veneer request is not a refusal of treatment but a re-sequencing of it: the underlying condition is treated first, and veneers are planned once the clinical foundations support a 10-year-plus service life. Patients redirected to a night guard, periodontal care, or orthodontics return as stronger candidates, and the lifespan figures quoted throughout this guide depend on exactly this selection discipline.
Why Choose Vera Smile for Long-Lasting Veneers
Vera Smile is an international dental clinic in Istanbul that focuses on durable, evidence-aligned veneer outcomes for patients travelling from abroad. Treatment planning prioritises the clinical factors that drive long-term survival rather than purely cosmetic shortcuts.
Patients choose Vera Smile for dental treatment in Turkey because the clinic combines:
- Turkish Ministry of Health authorisation: Full regulatory compliance for international dental treatment.
- Slow Dentistry Global Network standards: Proper isolation, time-controlled bonding, and disinfection protocols proven to support veneer longevity.
- AACD-aligned cosmetic expertise: Shade, shape, and smile-design precision built on accepted aesthetic criteria.
- Digital Smile Design on every full-arch case: Aesthetics and occlusion are aligned before any tooth is touched.
- 3D intraoral scanning and CAD/CAM dentistry: Marginal accuracy in the 20 to 50 micron range for a tighter cement seal.
- Transparent treatment planning: Written quotations, material disclosures, and lifespan expectations agreed in advance.
- International patient coordination: VIP airport transfers, accommodation coordination, and remote aftercare support that keep follow-up reliable after patients return home.
Patients receive a long-term maintenance plan together with their veneers, including night-guard recommendations where indicated and a structured remote check-in schedule.
FAQ
No. Younger patients retain veneers for similar durations to older adults, but they accumulate more lifetime replacement cycles. A patient veneered at age 25 should anticipate at least one and possibly two refit cycles across the remaining lifespan.
No. Full-coverage crowns generally outlast veneers because they distribute occlusal load across the entire tooth surface rather than across a thin bonded facing. Veneers remain the preferred option when the natural tooth structure is largely intact and the goal is conservative aesthetic improvement.
No. Clinical material and protocol matter more than geography. Veneer lifespan in Istanbul, London, or New York depends on the brand of ceramic, the bonding protocol, and the operator’s training, not on the country itself. Vera Smile supports returning international patients through its structured remote follow-up programme, with photo-based reviews after cementation, so that distance does not interrupt the six-month review cycle that protects veneer lifespan.
Yes. A single failed veneer can be replaced individually, although matching the shade and translucency of older neighbouring veneers becomes more difficult as the original set ages. Lab photographs taken at the original cementation help the technician reproduce the existing match.
No. Conventional porcelain and lithium disilicate veneers require enamel reduction, which is not reversible. No-prep veneers preserve enamel but are limited to specific case selections and do not suit all patients.