
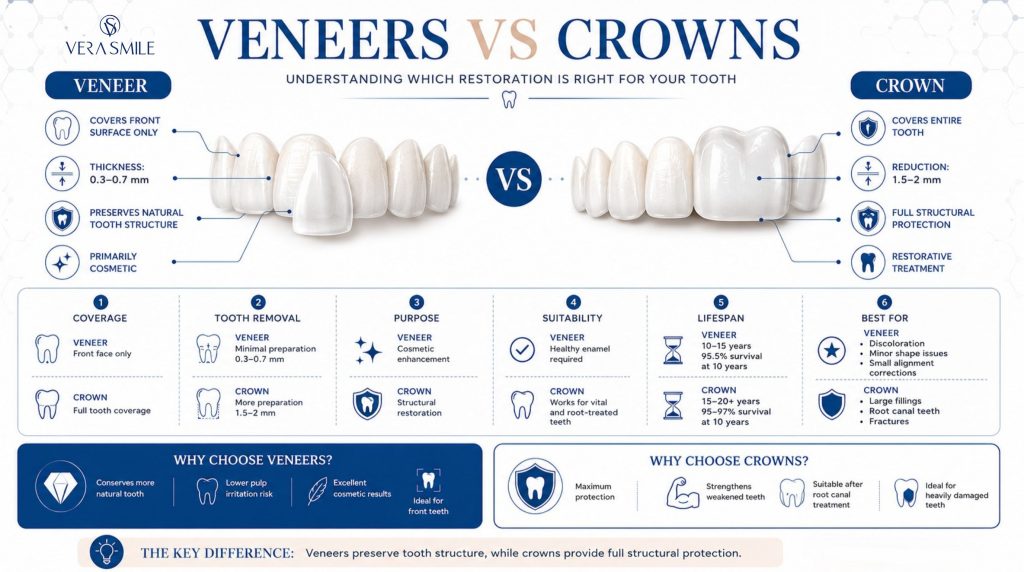
Veneers cover the front face of a tooth and treat cosmetic concerns such as discolouration, chips, and minor misalignment. Crowns cover the entire tooth and restore structural integrity after fracture, root canal therapy, or large fillings. Dentists remove 0.3 to 0.7 mm of enamel for a porcelain veneer and 1.5 to 2 mm on every surface for a crown. Porcelain veneers last 10 to 15 years; ceramic crowns last 15 to 20 years or more.
In the United States in 2026, veneers cost $925 to $2,500 per tooth and crowns cost $800 to $2,500, while a single tooth in Istanbul ranges from €100 to €375. Insurance often covers crowns and rarely covers veneers, because crowns are restorative and veneers are cosmetic. The two restorations look similar on a brochure but are not interchangeable, and matching the restoration to the diagnosis is what protects long-term survival.
What Is the Difference Between Veneers and Crowns?
A veneer is a thin shell that bonds to the front surface of a tooth, while a crown is a full-coverage cap that surrounds the entire visible tooth above the gumline. A dental veneer is made of porcelain, lithium disilicate, or composite resin, sits between 0.3 mm and 0.7 mm thick, and replaces only the visible enamel layer. A dental crown is made of ceramic, zirconia, lithium disilicate, or porcelain-fused-to-metal, and replaces enamel and a portion of dentin on every surface of the tooth.
The clinical decision rests on what the tooth has lost or risks losing. A tooth with intact enamel and an intact biting edge but a colour, shape, or alignment problem is a veneer case. A tooth that has been root-canal-treated, has a filling that exceeds half the tooth volume, or has a vertical fracture line is a crown case. The two restorations sometimes appear in the same mouth, on adjacent teeth, when one is structurally sound and the other is not.
How Do Veneers and Crowns Compare Across Key Variables?
Veneers and crowns differ across coverage, tooth removed, purpose, lifespan, risk, and cost, summarised in the comparison below. The single most consequential variable is how much tooth structure each restoration sacrifices.
| Variable | Porcelain Veneer | Ceramic / Zirconia Crown |
|---|---|---|
| Coverage | Front (labial) face only | All five surfaces, full cap |
| Tooth removed | 0.3 to 0.7 mm from front | 1.5 to 2 mm circumferentially |
| Primary purpose | Cosmetic | Restorative |
| Vital tooth required? | Yes, with healthy enamel | Vital or non-vital both possible |
| Reversibility | Practically irreversible (no-prep is the exception) | Irreversible |
| Lifespan (10-yr survival) | 95.5% | 95 to 97% |
| Lifespan (typical) | 10 to 15 years | 15 to 20 years or more |
| Risk of pulpitis | 2 to 3% | 11 to 19% on vital teeth |
| Insurance coverage | Rare (cosmetic class) | Common (50 to 80% restorative) |
| USA cost (2026, per tooth) | $925 to $2,500 | $800 to $2,500 |
| Turkey cost (2026, per tooth) | €175 to €375 | €100 to €400 |
| Front teeth suitability | First choice when intact | Secondary, for damaged teeth |
| Molar suitability | Rarely used | First choice |
The table shows the trade-off in one line: a veneer preserves tooth structure and carries lower pulpitis risk, while a crown sacrifices more tooth to deliver full structural protection.
How Much Tooth Is Removed for Veneers vs Crowns?
A porcelain veneer removes 0.3 to 0.7 mm of enamel from the front surface only, while a crown removes 1.5 to 2 mm of tooth structure from every surface. This is the variable competitors most commonly understate, and it is the difference that determines long-term survival.
For a porcelain veneer the dentist reduces 0.3 to 0.7 mm of enamel from the labial surface only. A small chamfer at the gum margin and a feather-edge at the incisal edge complete the preparation. Most preparations remain entirely within enamel, which is the substrate that produces the strongest adhesive bond and predicts the highest long-term survival.
For a crown the dentist reduces 1.5 to 2 mm from the front surface, 1.5 mm from the biting edge, and between 0.5 and 1.5 mm from the back and sides. The total volume of tooth structure removed for a single crown approaches eight times the volume removed for a veneer on the same tooth. Once removed, this tooth structure cannot be regenerated, which is why prosthodontists describe crown preparation as biologically expensive.
Why Is Enamel Loss Irreversible?
Enamel loss is permanent because adult enamel contains no living cells and cannot be deposited, repaired, or regrown. Every milimetre a dentist removes is gone for the lifetime of the patient. A 10-mm-tall central incisor that loses 1.5 mm of circumferential structure for a crown has surrendered roughly 30% of its supragingival volume. The same tooth prepared for a veneer has lost around 6%.
How Long Do Veneers vs Crowns Last?
Porcelain veneers reach a 10-year cumulative survival of 95.5%, and all-ceramic crowns reach approximately 95% at 10 years and 80 to 85% at 20 years. Manufacturer pages quote vague ranges of 5 to 25 years; the peer-reviewed evidence is more precise.
A retrospective cohort with 15-year follow-up reported a 93% success rate across 3,255 veneers. A 50-year follow-up of crown and veneer survival in a single dental practice (Friedman 2017, Journal of Prosthetic Dentistry) found that both restoration types maintained high survival when patients attended annual recall and maintained good oral hygiene.
Monolithic zirconia crowns, which carry the highest flexural strength of any current crown material, push the 10-year figure above 97% in adult patients without active bruxism. Porcelain-fused-to-metal crowns, the legacy option, survive at similar rates but show a higher chipping rate at the porcelain-to-metal interface and greater plaque accumulation at the metal margin.
Why Do Enamel-Bonded Veneers Outlive Dentin-Bonded Ones?
Veneers bonded to enamel survive at 99% (range 98 to 100%), while veneers bonded to severely exposed dentin drop to 91% (range 84 to 98%). Dentin contains tubules filled with fluid and a much higher protein component than enamel, which weakens the resin-tooth bond. A dentist who removes too much tooth structure during preparation does not only sacrifice volume; the restoration itself becomes less likely to survive.
How Much Do Veneers and Crowns Cost in 2026?
A single veneer costs €175 to €375 in Turkey and $925 to $2,500 in the United States, while a single crown costs €100 to €400 in Turkey and $800 to $2,500 in the United States. The figures below use 2026 data for a single-tooth indication, ceramic material, and an accredited provider.
| Market | Dental Veneer Cost (porcelain) | Dental Crown Cost (ceramic / zirconia) | Insurance friction |
|---|---|---|---|
| USA | $925 to $2,500 | $800 to $2,500 | Veneers excluded as cosmetic; crowns 50 to 80% covered up to annual maximum |
| UK (private) | £700 to £1,500 | £500 to £1,200 | Veneers private only; NHS Band 3 crown £326.70 (clinical-need only) |
| Canada | CAD $900 to $2,500 | CAD $1,000 to $2,500 | Cosmetic veneers excluded; crowns reimbursed by most plans |
| Turkey | €175 to €375 | €100 to €400 | All-inclusive package; no lab or imaging surprises |
In Istanbul, a full Hollywood Smile Turkey package of 16 to 20 teeth costs €2,500 to €5,000 and includes consultation, panoramic imaging, digital smile design, lab fees, and a one-week aftercare plan. The same volume of work in a US private practice routinely exceeds $30,000 before optional gum contouring and bite-guard fees are added.
How Are Veneers and Crowns Classified for Insurance?
Insurance carriers classify a restoration by clinical necessity, not appearance, so crowns are commonly reimbursed and veneers are commonly excluded. A crown placed on a tooth with a fractured cusp or after root canal therapy meets the medical-necessity threshold and triggers reimbursement of 50 to 80% up to the plan annual maximum (commonly $1,000 to $2,000 in the United States). A veneer placed on an intact tooth with a discolouration meets no medical-necessity standard and falls under the cosmetic exclusion. The same patient with the same plan can have one tooth restored at 80% reimbursement and the adjacent tooth at 0%, based on the diagnosis code submitted with the claim.
What Hidden Costs Are Excluded From a Headline Quote?
Headline quotes in the United States exclude several mandatory components that raise the final bill by 25 to 50%. The items below are the ones a patient should price before signing.
- Diagnostic wax-up: Adds $150 to $400 and is required to plan any multi-unit case.
- Digital smile design fee: Adds $500 to $1,500 for the planning and mock-up workflow.
- Provisional restorations: Add $75 to $200 per tooth for temporaries worn between visits.
- Occlusal night guard: Adds $300 to $700 and protects the restoration against grinding.
- Gingivectomy or crown-lengthening: Adds $400 to $1,000 per tooth when the gum line needs adjusting.
- Post-cementation occlusal adjustment: Adds $150 to $300 for the bite-balancing visit after delivery.
Added to the published per-tooth fee, a six-veneer smile makeover quoted at $9,000 routinely settles at $11,500 to $13,500 by the time the case is delivered. The Istanbul package price already contains these components, which is the basis of the cost difference.
What Are the Material Options for Veneers and Crowns?
Material choice drives strength, translucency, and final aesthetic, and the clinically meaningful figure is flexural strength in megapascals (MPa). The table compares the materials used at the clinic for veneers and crowns.
| Material | Flexural strength | Translucency | Best use |
|---|---|---|---|
| Composite resin (direct or indirect) | 80 to 120 MPa | Moderate | Budget veneers, single-tooth repairs |
| Feldspathic porcelain | 60 to 100 MPa | Highest | Anterior veneers, very thin laminates |
| Lithium disilicate (E-max) | 360 to 400 MPa | High | Anterior veneers and crowns, single-unit posterior crowns |
| Monolithic zirconia (BruxZir style) | 900 to 1,200 MPa | Lower | Posterior crowns, bridges, bruxism patients |
| High-translucency zirconia | 550 to 800 MPa | Moderate-high | Anterior crowns when strength matters |
| Porcelain-fused-to-metal | Framework-driven | Low (metal substrate) | Legacy posterior crowns, allergy-restricted cases |
E-max is the default ceramic for anterior veneers because its translucency mimics natural enamel light scattering, while zirconia is the default for posterior crowns because its strength tolerates the 600 to 900 N occlusal forces molars produce. The two are combined in a single mouth, with E-max veneers on the upper canines and central incisors and zirconia crowns on the molars.
When Should You Choose Veneers?
Veneers are the right choice when the tooth is structurally sound and the problem is cosmetic. The clinical indications below each define a veneer case.
- Intrinsic discolouration: Tetracycline staining, fluorosis, and internal trauma that does not respond to whitening are corrected with veneers.
- Small chips: Chips less than 2 mm in depth are resurfaced without full coverage.
- Peg-shaped or undersized laterals: Undersized lateral incisors are reshaped to match the arch.
- Mild rotation or crowding: Minor alignment issues the patient does not want to treat orthodontically are masked.
- Diastemas: Gaps up to 1 mm are closed with added porcelain width.
- Worn incisal edges: Mild attrition in patients with otherwise sound teeth is rebuilt.
Vera Smile clinicians require a digital smile makeover wax-up before any veneer case longer than four units. The wax-up is transferred to a putty index that becomes the in-mouth mock-up, and the patient wears the projected result for 7 to 14 days. A veneer plan the patient cannot live with for two weeks before the irreversible enamel reduction is a plan that needs revision.
When Should You Choose a Crown?
A crown is the right choice when the tooth has lost structural integrity or is at risk of losing it. The clinical indications below each define a crown case.
- Root-canal-treated teeth: Dehydration of pulpless dentin raises fracture risk by about 20%, so a crown is the standard protective restoration.
- Large fillings: Fillings exceeding 50% of the crown volume leave too little tooth to support a veneer.
- Vertical fracture lines: Cracks confined to the crown portion of the tooth are encircled and stabilised by a full cap.
- Severe attrition or erosion: Significant loss of clinical crown height is rebuilt with full coverage.
- Post-retained teeth: Endodontically treated teeth holding a post require a crown to distribute load.
A crown is also the final restoration on a dental implant. The titanium implant body integrates with bone, and a custom-milled zirconia or lithium disilicate crown is screwed or cemented onto the abutment, replacing the entire visible portion of the missing tooth. A single dental implant restores one missing tooth with this implant-and-crown combination rather than altering the healthy teeth on either side.
Are Veneers or Crowns Better for Front Teeth?
For front teeth the right restoration depends on what the tooth has lost, and an intact front tooth is a veneer case. Front teeth carry the highest aesthetic visibility and the lowest occlusal load. An intact upper central incisor with a tetracycline stain receives a porcelain veneer. The same incisor after a root canal and a 25-year-old composite filling covering 60% of the labial surface receives a crown.
Cosmetic dentists who reflexively crowned intact front teeth historically did so because crown preparations are easier to impress and fit. Adhesive dentistry has largely closed that gap. A modern intraoral scanner captures a 0.3 mm veneer preparation as accurately as a 1.5 mm crown preparation. The argument for crowning intact front teeth is weaker than it has ever been, and the long-term consequences of pulpitis risk and irreversible enamel loss remain identical.
Are Veneers or Crowns Better for Molars and Premolars?
For molars and premolars the crown is the correct choice in almost all cases, because these teeth absorb biting forces of 600 to 900 newtons. Lateral forces during grinding move the tooth into shear and torque states the thin labial surface of a veneer is not engineered to handle. Crowns dominate posterior dentistry because they encircle the tooth and absorb axial and lateral loads as a single piece of ceramic or zirconia.
The exception is the cosmetic case where a premolar is the most distal visible tooth in a smile (the second-premolar smile zone). In selected patients with low occlusal forces and no bruxism, a wraparound veneer covering the buccal surface and partially extending to the proximals is sometimes indicated. This is a niche, technique-sensitive restoration and not a substitute for a crown when a structural indication is present.
What Are the Risks of Veneers vs Crowns?
Both restorations carry complication profiles that practice websites tend to underplay, ranging from pulpitis to debonding. The figures below are the ones a patient should know before signing a treatment plan.
- Irreversible pulpitis: Occurs in 11 to 19% of vital teeth after full-coverage crown preparation versus 2 to 3% after an enamel-bonded veneer, driven by heat and dehydration during high-volume dentin reduction.
- Gingival inflammation from subgingival margins: Triggers chronic inflammation in 62% of cases at three years, with each millimetre of subgingival extension raising inflammation markers by about 40%.
- Veneer debonding: The most common veneer failure mode at 1 to 2% per year in the first 10 years, associated with bruxism, over-reduced preparations, and acid erosion from reflux.
- Crown chipping: Affects 2 to 8% of layered crowns at 10 years depending on material and bruxism, and is virtually eliminated by monolithic zirconia.
A crown that triggers irreversible pulpitis requires a root canal through the new restoration, which is possible but reduces case survival. Debonded veneers are re-cemented if the porcelain is intact and the tooth surface is clean; otherwise the veneer is remade.
When Do Patients Need Both Veneers and Crowns?
Patients need both when adjacent teeth differ in structural condition, which is common in a full upper smile makeover. A typical adult who comes to Vera Smile for a 10-tooth upper case often leaves with a plan that combines E-max veneers on the four incisors and two canines, E-max or zirconia crowns on the two premolars (often because of older fillings or root canals), and selective composite bonding to balance shape on the lower arch.
Mixing restorations across the same arch produces a more conservative final case than applying one solution to every tooth, and matching the restoration to the diagnosis protects long-term survival. Most of the clinics deliver combined cases through its Hollywood Smile Turkey package, which combines digital smile design, mock-up try-in, ceramic try-in, definitive bonding or cementation, and a finishing occlusal adjustment into a 5-to-7-day Istanbul stay.
Can You Get Veneers If You Already Have a Crown?
No. A porcelain veneer cannot bond to an existing crown, because the bonding chemistry depends on enamel and dentin substrate. The crown surface of zirconia, lithium disilicate, or porcelain-fused-to-metal does not develop the micromechanical and chemical interlock that produces a durable veneer bond. The clinical workaround is to remake the existing crown at the same time as the new veneers, with the new crown shaped, shaded, and surface-textured to match the veneer set. When the lab fabricates both restorations from the same digital wax-up, the colour and form match completely.
Can You Whiten Veneers or Crowns?
No. Whitening agents lighten natural enamel and dentin by oxidising chromogens within tooth structure, and ceramic veneers and crowns contain no organic chromogens. The bonded resin cement at the veneer margin can darken over years from coffee, red wine, and tobacco, which produces the appearance of a yellowing veneer, while the porcelain itself stays shade-stable. Composite resin veneers are the exception, because they are porous, take up surface stain, and require professional polishing every 12 to 18 months to maintain shade.
Patients planning veneers or crowns should whiten their natural teeth first, allow the shade to stabilise for 14 days, and then take a final shade reference for the lab. This sequence prevents the post-treatment mismatch that occurs when the natural teeth lighten after the ceramic has been milled.
Why Patients Choose Vera Smile in Istanbul for Veneers and Crowns
Vera Smile is an internationally accredited dental clinic in Istanbul, Türkiye, operating under Republic of Türkiye Ministry of Health authorisation and as a member of the Slow Dentistry Global Network, which enforces measured treatment timelines, sterilisation standards, and patient-first protocols. Clinical work follows guidelines aligned with the American Academy of Cosmetic Dentistry, and the editorial and treatment teams maintain a commitment to scientific excellence and continuous research that anchors how each case is planned, documented, and reviewed.
Vera Smile treatment packages combine every cost component into a single transparent figure: 3D intraoral scanning, digital smile design, panoramic and CBCT imaging, lab fees for E-max or zirconia, ceramic try-in, definitive cementation, an occlusal night guard, and remote 1-week and 4-week video follow-up. Patients receive a written aftercare protocol in English and a documented emergency contact line for the recovery period. VIP airport-to-clinic transfer and accommodation coordination are included on request.
Patients whose case extends beyond cosmetic veneers and crowns (dental implants in Turkey, All-on-4 dental implants, full-arch reconstruction, or single dental implant placement) consolidate every step into one Istanbul visit. The 5-to-7-day treatment compression is what removes the second airfare and the second hotel cost from the total of care.
FAQ
Yes. Bruxism increases the failure rate of both restorations by 2 to 4 times depending on severity. Patients with active bruxism receive a hard acrylic occlusal guard at delivery and are advised to wear it nightly for the lifetime of the restoration. Untreated bruxism is the single most preventable cause of porcelain fracture, debonding, and chipping in the first 5 years.
Traditional porcelain veneers are not reversible, because the dentist removes 0.3 to 0.7 mm of enamel that does not regenerate. No-prep veneers such as Lumineers preserve nearly all enamel and are technically reversible, because the cement can be removed with limited damage. No-prep designs work best on small or undersized teeth and do not work for oversized teeth or teeth that need to be made smaller.
Indirectly, yes. A subgingival crown or veneer margin that extends into the sulcus provokes chronic inflammation in approximately 62% of cases, and prolonged inflammation drives recession over years. A supragingival or equigingival margin placed on a stable periodontal biotype does not cause recession. The decision belongs to the dentist, not the material.
A crown is the standard of care after root canal therapy on a posterior tooth and is recommended on most root-canal-treated anterior teeth. Endodontically treated teeth are more brittle than vital teeth, with an estimated 20% reduction in fracture resistance, and a crown distributes occlusal load to reduce fracture risk. Veneers are sometimes placed on root-canal-treated front teeth with minimal access cavity preparation and intact lingual structure, but the default protocol is a crown.
A full Hollywood Smile package combining 16 to 20 E-max veneers and zirconia crowns in Istanbul, Turkey costs €2,500 to €5,000 in 2026 and includes consultation, panoramic and CBCT imaging, digital smile design, ceramic try-in, definitive cementation, an occlusal night guard, and 5-star hotel accommodation with airport transfers. The same case in a US private practice costs $30,000 to $45,000 once lab fees, smile design, and night guards are included, making the all-in cost 60 to 75% lower in Istanbul.
In the 20-to-30 age group, the right answer is whichever restoration matches the diagnosis on the specific tooth. A 24-year-old with intact teeth and a tetracycline stain receives veneers, because the tooth structure is sound and as much enamel as possible should be preserved for the next 60 years. A 28-year-old with a fractured upper first molar after a sports injury receives a crown, because the tooth has lost structural integrity. Age alone is not a decision variable.