
Gum recession, also called gingival recession or receding gums, is the gradual loss of gum tissue from the visible neck of the tooth, exposing the cementum-covered root surface. It is highly prevalent. NHANES data report at least one site of recession of 1 mm or more in around 58% of adults over 30, rising with age. The leading causes are periodontal disease, mechanical trauma from aggressive brushing, occlusal trauma from bruxism, smoking, orthodontic movement, and an inherited thin gingival biotype.
Recession is classified clinically using the Miller (1985) or the newer Cairo (2011) system, which guide treatment planning. Treatment ranges from technique correction and composite root coverage for mild cases to connective tissue grafting, free gingival grafting, or the pinhole surgical technique for moderate to severe cases. Recession also affects planning for cosmetic and restorative work, including dental veneers and dental crowns.
What Is Gum Recession?
Gum recession is the apical (downward) migration of the gingival margin from its natural position at the cement-enamel junction, exposing the root surface of the tooth. The exposed root is more porous than enamel, less wear-resistant, and not naturally adapted to oral exposure.
Two anatomical points define the recession:
- Cement-enamel junction (CEJ): The line where the crown enamel meets the root cementum, where the gum margin normally sits at or slightly above.
- Free gingival margin: The visible edge of the gum tissue against the tooth; when it moves below the CEJ, recession is present.
Recession can affect a single tooth (localised) or multiple teeth in an arch (generalised). It can occur on the facial (cheek-side), lingual (tongue-side), or interproximal (between teeth) surface. Most clinically significant recession is facial, especially of canines and premolars.
Clinical note: Recession is measured from the cement-enamel junction to the gingival margin in millimetres. A 1 to 2 mm recession is mild, 3 to 4 mm moderate, and 5 mm or more severe. Depth, width, and the presence of interproximal bone loss all influence the treatment plan.
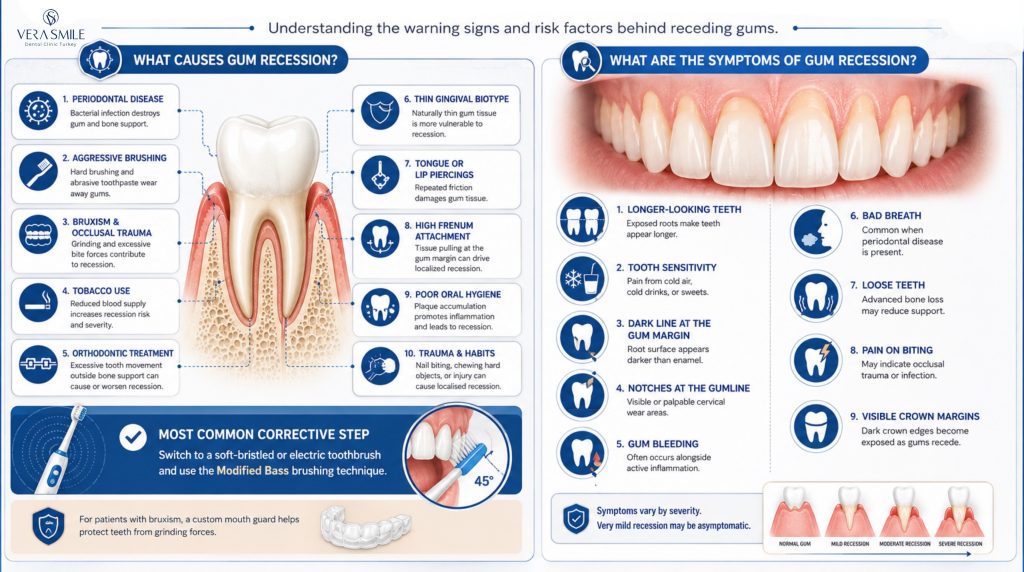
What Causes Gum Recession?
Gum recession is caused by mechanical trauma, periodontal infection, occlusal overload, anatomical predisposition, and a small set of lifestyle and orthodontic factors. Most cases result from a combination of two or more of these drivers, not a single cause.
- Periodontal disease: Bacterial inflammation of the gum and bone is the leading cause in adults, destroying the periodontal ligament and bone so the soft tissue follows.
- Aggressive brushing: Hard-bristled brushes, abrasive toothpaste, and a horizontal scrubbing technique abrade the gum margin over years.
- Bruxism and occlusal trauma: Heavy grinding transmits force to the cervical area of the tooth, contributing to recession and to non-carious cervical lesions at the gum line.
- Tobacco use: Smoking impairs gum tissue blood supply and increases recession risk and severity.
- Orthodontic treatment: Moving teeth outside the alveolar bony envelope, particularly during expansion or proclination, can produce or worsen recession.
- Thin gingival biotype: A genetically thin, scalloped gum tissue is more susceptible to recession than a thick, flat biotype.
- Tongue or lip piercings: Direct mechanical irritation against the anterior teeth causes localised recession.
- High frenum attachment: A frenum that pulls on the gum margin can drive localised recession.
- Poor oral hygiene: Plaque accumulation drives gingivitis and progresses to recession over time.
- Trauma: Direct impact or chronic habits such as nail biting and chewing hard objects produce localised recession.
The most common single corrective step is switching to a soft-bristled or electric brush with a modified Bass technique. For patients with diagnosed bruxism, a custom mouth guard for grinding teeth addresses the occlusal component.
What Are the Symptoms of Gum Recession?
The most common symptoms of gum recession are visible root exposure, tooth sensitivity to cold or sweet, a dark line at the gum margin, and notches felt at the gumline. Symptoms vary by severity, and very mild recession may be asymptomatic.
- Longer-looking teeth: The exposed root makes the tooth appear longer than its neighbours.
- Tooth sensitivity: Sharp pain on cold air, cold drinks, or sweet foods, caused by exposed dentine tubules at the root surface.
- Dark line at the gum margin: Root cementum and exposed dentine are darker than enamel, producing a visible margin line.
- Notches at the gumline: Cervical wear or non-carious cervical lesions felt with the tongue or fingernail.
- Gum bleeding on brushing: Often present when active periodontal inflammation accompanies recession.
- Bad breath: Common when periodontal disease is part of the cause.
- Loose teeth: Seen in advanced cases where bone loss has compromised tooth support.
- Pain on biting: Less common, and usually associated with occlusal trauma or a periodontal abscess.
- Visible exposed crown margins: A common late sign on teeth with existing crowns, where the dark cement line or metal substructure becomes visible.
How Is Gum Recession Diagnosed?
Gum recession is diagnosed by clinical examination, periodontal probing, photographic records, and classification using the Miller or Cairo system. Radiographs assess interproximal bone loss, which determines whether root coverage is achievable.
- Visual inspection: Identifies the location, severity, and pattern of recession.
- Periodontal probing: Measures recession depth from CEJ to gingival margin, pocket depth, and clinical attachment level around each tooth.
- Keratinised tissue assessment: Measures the band of attached gum between the recession line and the mucogingival junction, where less than 2 mm is a risk factor.
- Photographic records: Standardised intraoral photographs document baseline and track progression.
- Periapical and bitewing X-rays: Identify interproximal bone loss, which affects whether root coverage is biologically possible.
- Cone beam CT (CBCT): Used in complex or pre-surgical cases to assess buccal bone thickness.
A periodontal assessment of this kind is delivered through periodontics, which combines probing, imaging, and classification into a single written diagnosis.
How Is Gum Recession Classified?
Gum recession is classified using the Miller (1985) system or the Cairo (2011) system, both of which predict how much root coverage is achievable. The Miller system sorts recession into four classes:
- Class I: Recession does not reach the mucogingival junction with no interproximal tissue loss, and 100% root coverage is achievable.
- Class II: Recession extends to or beyond the mucogingival junction with no interproximal tissue loss, and 100% root coverage is achievable.
- Class III: Interproximal tissue loss is present but less severe than the buccal recession, allowing partial root coverage only.
- Class IV: Severe interproximal tissue loss equal to or greater than the buccal recession, where root coverage is not achievable.
The Cairo system is the modern alternative, using three Recession Types (RT1, RT2, RT3) based on interproximal clinical attachment level. It is increasingly preferred in published literature because it relies on objective measurements rather than visual landmarks.
Is Gum Recession Reversible?
No, gum recession is not spontaneously reversible. Lost gingival tissue does not regenerate on its own, and surgical grafting is the only way to restore lost tissue and root coverage. Non-surgical management can halt progression and address symptoms, but cannot replace lost tissue.
Key fact: When patients ask whether gum recession can be reversed without surgery, the honest clinical answer is no for the visible tissue loss and yes for the underlying disease progression. Stopping further loss is realistic, and regrowth is not.
What Are the Treatment Options for Gum Recession?
Treatment of gum recession is determined by severity, the underlying cause, the Miller or Cairo class, and the patient’s aesthetic and functional priorities. It ranges from technique correction for mild cases to surgical grafting for moderate to severe cases.
| Severity | Recommended treatment | Expected outcome |
| Mild (1 to 2 mm), no symptoms | Brushing technique correction, soft brush, desensitising paste | Halts progression; cosmetic change minimal |
| Mild with notches (NCCL) | Composite restoration of cervical lesions | Functional and aesthetic improvement |
| Moderate (3 to 4 mm), Miller I or II | Connective tissue graft, pinhole technique, or coronally advanced flap | Complete or near-complete root coverage |
| Moderate to severe with thin biotype | Free gingival graft or CTG with tissue engineering | Increased keratinised tissue and root coverage |
| Severe (Miller III or IV) | Partial coverage graft or restorative camouflage | Partial coverage only; aesthetic and biological improvement |
| Recession with active periodontitis | Periodontal therapy first, then grafting | Disease control before tissue regeneration |
The pre-surgical step in nearly every case is technique correction and plaque control. Surgery on an uncontrolled periodontal background fails predictably.
What Is Gum Graft Surgery?
Gum graft surgery is a periodontal procedure that treats gum recession by covering exposed tooth roots with donor tissue, restoring the gumline and increasing the amount of attached gum tissue. The most common technique is the connective tissue graft (CTG), considered the gold standard for its predictable aesthetic and functional results.
Other options include free gingival grafts, pedicle grafts, and acellular dermal matrix (ADM) grafts, depending on the patient’s needs. Initial healing takes around two weeks, while full tissue maturation requires three to six months.
What Is the Pinhole Surgical Technique for Gum Recession?
The Pinhole Surgical Technique (PST) is a minimally invasive procedure developed by Dr. John Chao, in which gum tissue is repositioned over the exposed root through a small pinhole-sized entry point, with no scalpel incisions and no sutures. It uses collagen membranes to stabilise the repositioned tissue.
- Minimally invasive: A single small pinhole entry per area treated, with no cutting of the gum margin.
- No suturing: Stability is achieved by collagen membrane placement and natural tissue tension.
- Multiple teeth in one visit: Several teeth or an entire arch can be treated in a single appointment.
- Faster recovery: Soft-tissue healing in around 1 week, compared with 2 to 3 weeks for conventional grafting.
- Limitations: Best for Miller Class I and II cases, since severe recession or thin biotype may still require conventional grafting.
The PST repositions existing tissue and does not introduce new keratinised tissue. When keratinised tissue is inadequate, a CTG remains the more reliable option.
Clinical note: The pinhole technique is technique-sensitive and operator-dependent. Outcomes in published clinical series are comparable to conventional grafting when performed by experienced clinicians on appropriately selected cases.
How Much Does Gum Recession Treatment Cost in Turkey?
Gum recession treatment costs in Istanbul range from €200 for cervical composite restoration of a single tooth to €1,800 or more for connective tissue grafting of multiple teeth. International patient packages may include accommodation and transfers.
| Treatment | Price range (Istanbul) | Notes |
| Brushing technique correction and review | €60 to €120 | Hygiene visit, often the only intervention needed for early recession |
| Composite restoration of cervical lesion | €100 to €200 per tooth | Restores the notch and reduces sensitivity |
| Scaling and root planing (full mouth) | €200 to €450 | Periodontal therapy when active disease is present |
| Pinhole Surgical Technique (per arch) | €1,200 to €2,500 | Multiple teeth in one visit |
| Connective tissue graft (per site) | €400 to €800 | Gold standard for Miller I and II cases |
| Free gingival graft (per site) | €350 to €700 | Used to increase keratinised tissue |
| Acellular dermal matrix graft (per site) | €500 to €900 | Avoids palatal harvesting |
These ranges are approximate for international patients and vary by case complexity, the number of sites treated, and any pre-treatment periodontal work needed.
How Can You Prevent Gum Recession?
The most effective prevention strategies for gum recession are correcting brushing technique, treating periodontal disease early, managing bruxism, stopping tobacco use, and attending six-month periodontal reviews. Most cases develop gradually, which means most are preventable.
- Switch your brush: Use a soft-bristled or electric brush with a sensitive head and an oscillating or sonic action.
- Correct your technique: Use the modified Bass technique with gentle 45-degree angled short strokes, not horizontal scrubbing.
- Lower abrasion: Choose a low-abrasive toothpaste (RDA below 100) to reduce cervical wear.
- Clean between teeth: Floss daily or use interdental brushes to remove plaque between teeth.
- Attend reviews: Six-month professional cleanings let the dentist identify early recession before it becomes visible to the patient.
- Treat disease early: Address periodontal disease promptly when bleeding or pocket depth is identified.
- Manage grinding: Wear a night guard if bruxism is present to reduce occlusal force on the cervical area.
- Quit smoking: Stopping tobacco restores gum tissue blood supply and lowers recession progression.
- Set orthodontic limits: Discuss boundaries with the treating dentist or orthodontist so expansion or proclination stays within the bony envelope.
- Address piercings: Remove tongue or lip piercings if they are causing localised recession.
Patient tip: A single dental hygiene visit that reviews brushing technique often produces the largest single reduction in recession progression. Patients who have brushed aggressively for decades benefit most from technique correction with photographic feedback.
How Does Gum Recession Affect Dental Treatment?
Gum recession affects veneer placement, crown longevity, implant survival, and aesthetic outcomes by changing the margin position, exposing dentine, and reducing the keratinised tissue band that protects restorations. It is one of the most important variables a clinician assesses before treatment with dental implants or cosmetic restorations.
- Veneer planning: Recession exposes root surface, which does not bond to porcelain as reliably as enamel, so margins may need to sit above the recession line.
- Crown margins: Recession exposes existing crown margins, producing a dark gum-line and increasing recurrent caries risk, which often requires replacement.
- Implant placement: Keratinised tissue around implants supports long-term peri-implant health, so recession near a planned site is corrected with grafting before or during surgery.
- Aesthetic smile design: Uneven gum lines produce a stepped or asymmetric smile that cosmetic dentistry must address before veneer or crown work.
- Sensitivity management: Exposed root surfaces are more sensitive after restorative work, particularly during preparation under local anaesthesia.
- Bridge planning: Recession around bridge abutments may compromise the seal and require pre-treatment grafting.
- Older patient planning: Recession is more prevalent in older adults, which influences material choice and margin design.
A comprehensive treatment plan addresses recession before cosmetic or restorative work begins, not after.
How Do Digital Workflows Improve Gum Recession Treatment?
Digital workflows improve gum recession treatment through 3D intraoral scanning, photographic monitoring, and Digital Smile Design integration that aligns periodontal correction with the planned aesthetic outcome. They do not replace surgical skill, but they reduce planning errors and improve patient communication.
- 3D intraoral scanning: Captures the soft-tissue contour at high accuracy for baseline records and post-surgical comparison.
- Photographic monitoring: Records progression over time with standardised lighting and angle.
- Digital Smile Design preview: Shows the planned gum margin position alongside the planned tooth shape, aligning periodontal surgery with the cosmetic outcome.
- Digital sequencing: Presents which periodontal corrections come before restorative work, so the patient understands the order.
FAQ
No. Lost gingival tissue does not regenerate spontaneously. Non-surgical management can stop progression and reduce symptoms, but tissue regrowth requires surgical grafting. Marketing claims about herbal treatments or mouthwashes that regrow gums are not supported by clinical evidence.
Progression varies. Slow progression of 0.1 to 0.3 mm per year is common in patients with controlled periodontal status and good brushing technique. Faster progression occurs when active periodontal disease, severe bruxism, or aggressive brushing is uncontrolled. Documented progression over 6 to 12 months warrants intervention.
Often, but not always. Recession can occur without periodontal disease, particularly when caused by aggressive brushing, bruxism, or orthodontic movement. A clinical examination with periodontal probing distinguishes recession with active disease from recession with healthy gums but compromised tissue thickness.
No. Mild recession with no symptoms and no active disease is managed with technique correction, hygiene optimisation, and six-month review. Surgery is reserved for moderate to severe cases, aesthetic concern, persistent sensitivity, or cases where recession threatens tooth survival or planned restorative work.
Soft-tissue healing takes around 2 weeks. Most patients return to normal eating within 1 to 2 weeks. Full biological maturation of the graft site takes 3 to 6 months. Patients can usually fly home 1 to 3 days after surgery, and the dental team coordinates a remote follow-up schedule for international patients.
Yes, in advanced cases. Severe recession combined with bone loss compromises the periodontal support of the tooth and increases the risk of mobility and eventual loss. Early intervention to halt recession and stabilise periodontal status is the most effective tooth-preservation strategy.
Yes, in most cases, although the recession site is usually grafted first to rebuild the keratinised tissue band that protects the implant. Vera Smile assesses candidacy on a case-by-case basis, as set out for patients considering dental implants with receding gums.