
A crowned tooth can still become infected because the crown covers only the visible part of the tooth and does not seal the root, the surrounding bone, or the gum. An infection under a dental crown starts when bacteria reach the pulp or the tissue around the root tip through a failing crown margin, secondary decay, a cracked root, or diseased gum tissue. Symptoms range from a persistent bad taste and mild biting pain to spontaneous throbbing, gum swelling, and a draining pimple on the gum. Treatment depends on whether the infection is inside the tooth (pulpal) or in the surrounding gum (periodontal): a pulpal infection needs root canal treatment or extraction, while a gum infection is treated with deep scaling and drainage. Facial swelling, fever, or a swollen jaw signals that the infection has spread and requires emergency care the same day.
Can a Tooth with a Crown Get Infected?
Yes. A crowned tooth can still develop an infection. The crown protects the visible part of the tooth but does not seal the root, the surrounding bone, or the gum tissue. Bacteria enter through a failing crown margin, secondary decay under the crown, a cracked root, or the gum tissue. Once bacteria reach the pulp chamber or the periapical tissue around the root tip, an infection, and potentially an abscess, forms.
Crowns are often mistaken for a definitive fix. The tooth is capped, the pain from the original damage is gone, and most patients assume it is protected permanently. That assumption is mostly right, but not entirely.
A dental crown covers the tooth above the gumline, while the root sits in the bone below. The pulp, the living nerve and blood supply inside the tooth, remains intact unless a root canal has already been performed. If bacteria reach that pulp, they cause an infection just as easily in a crowned tooth as in a natural one.
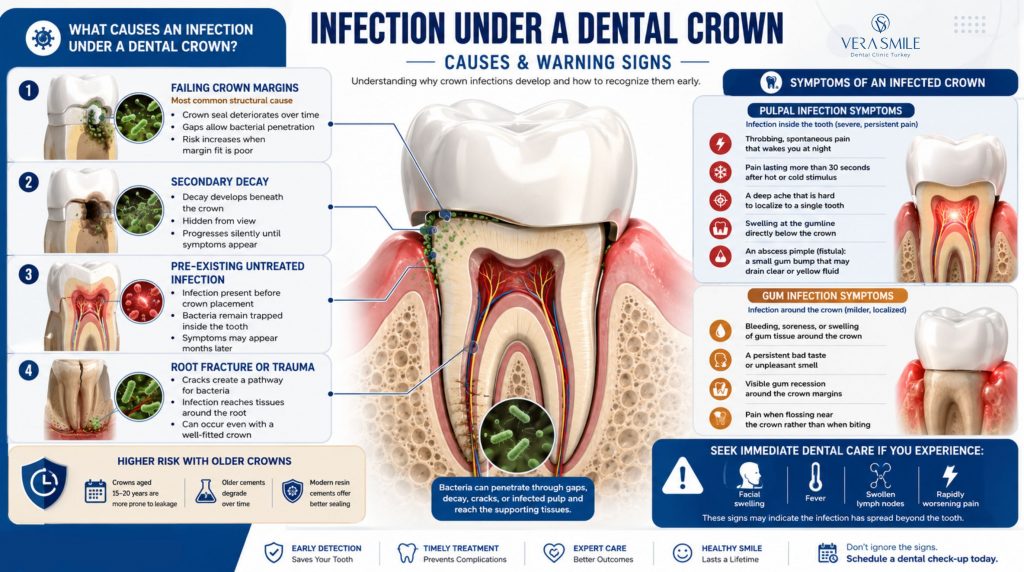
What Causes an Infection Under a Dental Crown?
The four main causes of a crown infection are a failed or leaking crown margin, secondary decay under the crown, a pre-existing infection that was not resolved before the crown was placed, and a root crack or trauma that lets bacteria reach the periapical tissue. A poor crown fit, specifically a margin gap greater than 100 micrometers, is the most common structural cause.
The main causes break down as follows:
- Failing crown margins: The seal between crown and tooth degrades over time, and a 2018 Journal of Prosthetic Dentistry study found that margin gaps exceeding 100 micrometers allow significant bacterial penetration within 6 months of cement degradation.
- Secondary decay: Natural tooth structure decays once bacteria work through a compromised margin, and the process progresses silently because it is hidden beneath the porcelain.
- Pre-existing untreated infection: A tooth crowned over a compromised pulp, often to avoid a root canal, traps bacteria that continue to multiply, which is a common reason infections appear months after placement.
- Root fracture or trauma: A crack extending into the root creates a direct bacterial pathway to the periapical tissue, and this can occur even with a well-fitted crown.
Infection risk rises sharply with crown age. A crown placed 15 to 20 years ago with conventional zinc phosphate or glass ionomer cement is far more likely to have leaking margins than one placed with modern resin cement and digital margin fitting.
What Are the Symptoms of an Infected Crown?
The key symptoms of an infected dental crown are spontaneous throbbing pain (worse at night), pain that lingers more than 30 seconds after hot or cold contact, gum swelling near the crown, a persistent bad taste or smell, a pimple-like bump on the gum (a dental fistula), and sensitivity to biting. Fever, facial swelling, or swollen lymph nodes mean the infection has spread and require immediate emergency care.
The symptom pattern depends on whether the infection is inside the tooth (pulpal) or in the surrounding gum and bone (periodontal). The two present differently.
Pulpal Infection Symptoms
Pulpal symptoms come from inside the tooth and root and tend to be severe and poorly localised.
- Throbbing, spontaneous pain that wakes you at night.
- Pain lasting more than 30 seconds after a hot or cold stimulus.
- A deep ache that is hard to localise to a single tooth.
- Swelling at the gumline directly below the crown.
- An abscess pimple (fistula): a small gum bump that may drain clear or yellow fluid.
Gum Infection Symptoms
Gum symptoms appear around the crown margin and are usually milder than pulpal pain.
- Bleeding, soreness, or swelling of gum tissue specifically around the crown.
- A persistent bad taste near the crown, often described as metallic or salty.
- Visible gum recession around the crown margin.
- Pain when flossing near the crown rather than when biting.
Symptom Triage Table
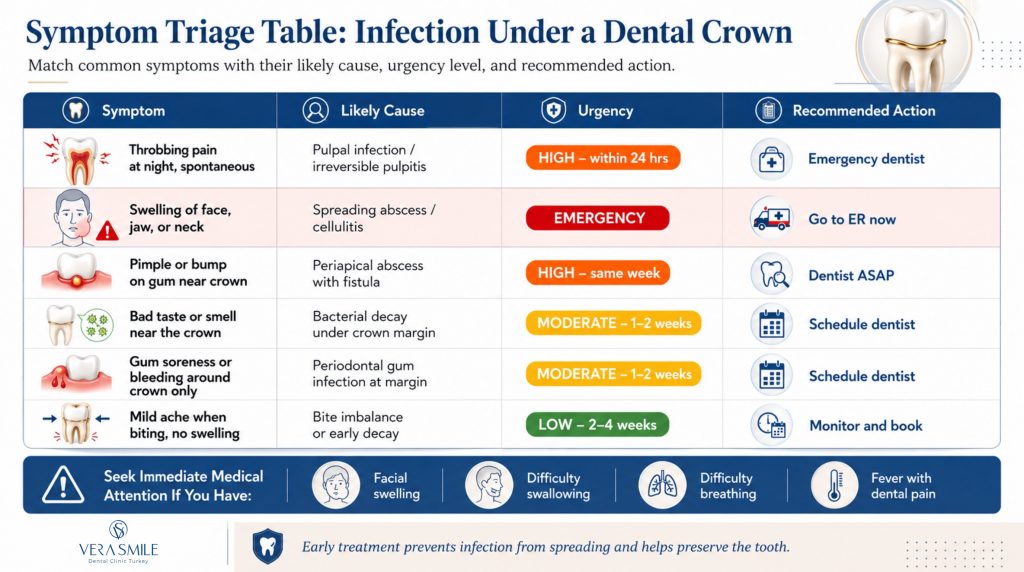
Any symptom in the EMERGENCY or HIGH band should not be left to monitor, even if the pain eases on its own.
Can a Tooth Actually Rot Under a Crown?
Yes. A tooth can decay under a crown when bacteria penetrate a leaking margin. The decay forms on the natural tooth structure beneath the crown, stays invisible on the surface, and is often undetectable without X-rays, so by the time symptoms appear it may already have reached the pulp. This is called recurrent or secondary caries and is a leading cause of crown failure, affecting an estimated 11 to 16% of crowns within 10 years (Journal of Evidence-Based Dental Practice, 2019).
When the cement seal between crown and tooth fails, sugar and acid from food and drink seep into the gap. The dentine underneath is softer than enamel and decays faster, and because it is hidden under the crown neither you nor your dentist can see it without a bitewing X-ray.
By the time secondary caries causes pain, sensitivity, or visible breakdown at the margin, it often extends into the pulp chamber. At that point the choice narrows to root canal treatment to save the tooth or extraction.
This is why dental X-rays every 12 to 18 months matter even for crowned teeth. A small cavity caught at the margin is a filling, while the same cavity found two years later is a root canal.
What Is the Difference Between a Crown Infection and an Abscess?
A crown infection is any bacterial infection in or around a crowned tooth, whether in the pulp, the periapical tissue, or the gum. An abscess is a pocket of pus that forms when the immune system walls off that infection: a periapical abscess forms at the root tip, and a periodontal abscess forms in the gum pocket beside the tooth. Both need professional treatment, and neither resolves on its own.
A periapical abscess sits at the tip of the root and follows pulp death, when bacteria kill the nerve, travel down the canal, and trigger an immune response in the bone. Resolving it requires a root canal or extraction, because antibiotics reduce spread but do not remove the source.
A periodontal abscess sits beside the root inside the gum pocket or bone and is driven by gum disease bacteria, not pulp death. The tooth itself may be healthy internally, and treatment involves scaling the root surface, draining the abscess, and sometimes surgery if bone loss is advanced.
A crowned tooth can develop either type, or both at once. The dentist determines which is present using X-rays, percussion testing, and probing depth measurements.
How Do You Treat an Infected Dental Crown?
Treatment depends on whether the infection is pulpal or periodontal. A pulpal infection needs root canal treatment through the crown, or crown removal followed by a root canal and a new crown. A periodontal infection needs deep scaling and root planing, antibiotics, and sometimes gum surgery. In severe cases such as a vertical root fracture, extensive secondary decay, or systemic spread, extraction is the only option. Antibiotics alone never cure a dental infection.
The main treatment options are:
- Root canal through the existing crown: If the crown is well-fitted and undamaged, the dentist drills an access hole, performs the root canal, and seals the hole so the crown stays in place.
- Crown removal, root canal, and new crown: If the crown has failing margins or secondary decay, it is removed before the root canal, a temporary crown protects the tooth, and a new permanent crown is placed once the infection resolves after 2 to 4 weeks.
- Deep scaling for periodontal infection: When the infection is in the gum around the crown, professional teeth scaling removes the bacterial biofilm from the root surface, followed by antibiotics and, where bone loss has occurred, possible gum surgery.
- Extraction: When the root is fractured vertically, too little tooth structure remains to restore, or the infection has spread irreversibly into the bone, the tooth is removed and later replaced with an implant or bridge.
The right option depends on the crown’s condition and how far the infection has reached, which the dentist confirms with X-rays before treatment begins.
Does an Infected Crown Always Need a Root Canal?
No. An infected crown does not always need a root canal. A gum infection around the crown margin (periodontal abscess) is treated with scaling, drainage, and antibiotics. A pulpal infection, where bacteria have reached the nerve tissue inside the root, always needs either a root canal or extraction, because there is no other way to eliminate the bacterial source inside the root canal system.
Patients often hope antibiotics will resolve a tooth infection without a root canal. That is understandable but incorrect for pulpal infections. Antibiotics travel in the bloodstream, and once the pulp dies there is no blood supply inside the canal for them to reach. They can reduce the spreading infection in the surrounding bone and tissue, which is why they are prescribed, but the infection returns as soon as the course finishes unless the root is cleaned.
Can Antibiotics Alone Cure a Crown Infection?
No. Antibiotics manage the spread of infection but do not eliminate the source. In a pulpal infection the bacterial reservoir inside the root canal cannot be reached by blood-borne antibiotics because the dead pulp is no longer vascular. Antibiotics are prescribed to prevent systemic spread, reduce acute symptoms, and protect against Ludwig’s angina or fascial space infection in high-risk cases, not as a standalone cure.
Amoxicillin 500mg three times daily or metronidazole 400mg three times daily are the most commonly prescribed antibiotics for dental infections in the US and UK. They are appropriate alongside treatment, not as replacements for it.
The one exception is when facial swelling is present and the patient is systemically unwell. In that scenario intravenous antibiotics in hospital take priority over immediate dental treatment, buying time for swelling to reduce before the dentist can safely operate.
Medically compromised patients (immunosuppressed, on blood thinners, or with cardiac valve conditions) need early antibiotic cover before dental procedures, discussed with both the treating dentist and the patient’s physician.
What Happens If You Leave a Crown Infection Untreated?
An untreated crown infection progresses in stages. Within days to weeks the abscess grows and may form a fistula (a draining sinus) on the gum, which relieves pain temporarily but does not resolve the infection. Within weeks to months the infection spreads into the surrounding jawbone (osteomyelitis). In rare but documented cases it spreads to the floor of the mouth, neck, or airway, a condition called Ludwig’s angina that carries a mortality rate of up to 10% without immediate surgical treatment (JAMA, 2020).
How Long Does It Take for a Crown Infection to Develop?
A crown infection can develop at any point, from days after placement (if a pre-existing infection was not resolved first) to 10 to 15 years later as margins degrade and secondary decay sets in. A flare within the first 2 to 8 weeks usually points to incomplete pulp assessment before crowning, while an infection appearing years later reflects margin failure or new decay.
The timing tends to follow a pattern:
- Days to weeks after placement: Almost always a pre-existing condition is missed before cementing, because the trauma of crown preparation can tip a compromised pulp into irreversible pulpitis.
- 3 to 18 months after placement: Often a poorly fitted margin or inadequate seal allowing bacterial entry from the start, which the 12-month bitewing review should catch.
- 3 to 10 years after placement: Cement failure, margin wear, or gum recession exposing the margin, which is a biological reality in ageing crowns rather than necessarily poor workmanship.
- 10+ years after placement: Expected in older crowns, especially those placed with zinc phosphate cement, where regular X-ray monitoring should detect secondary decay before it reaches the pulp.
In short, an early flare points to a problem present before crowning, while a late one reflects the gradual breakdown of the margin seal.
What Is the 3-3-3 Rule for Tooth Infection?
The 3-3-3 rule is a clinical guideline for monitoring antibiotic response: you should see significant improvement within 3 days of starting antibiotics, the infection should be resolved (with dental treatment) within 3 weeks, and an infection left untreated for 3 months risks chronic bone involvement and systemic complications. If symptoms are not clearly improving after 3 days on antibiotics, contact your dentist, because the antibiotic may be wrong or the source may need immediate drainage.
Each stage matters for a specific reason:
- 3 days: Swelling should be reducing and pain easing, and if it is not, the case needs escalation rather than more waiting.
- 3 weeks: With appropriate treatment (root canal, scaling, or extraction) the acute infection should be gone, even though bone healing continues for months.
- 3 months: The point at which an untreated infection risks crossing from acute to chronic, with progressive bone loss, fistula formation, and higher treatment complexity.
The rule is a monitoring aid, not a treatment plan: definitive dental treatment still has to remove the source of the infection within that window.
How Can You Prevent an Infection Under a Dental Crown?
Most crown infections are preventable, because they develop when small problems go undetected long enough to become large ones. The measures below address the crown margin, where the risk concentrates.
- Floss daily at the crown margin: The junction between crown and tooth is the most vulnerable point, and floss threaders, water flossers, or interdental brushes disrupt the biofilm before it causes decay.
- Do not skip check-up X-rays: Secondary decay under a crown is invisible to the naked eye, so bitewing X-rays every 12 to 18 months catch it early; patients who skip imaging for 3 to 4 years are the ones who present with advanced infections.
- Watch for early warning signs: A persistent bad taste, returning sensitivity in a previously settled crowned tooth, or gum changes at the margin all warrant an appointment.
- Replace ageing crowns proactively: A crown placed 15 or more years ago with older cement is a candidate for renewal before symptoms develop, especially if cleaning reveals margin staining or recession.
Together these habits protect the margin seal, which is the single point where most preventable crown infections begin.
Why Do Vera Smile Crowns Have Lower Infection Risk?
Vera Smile crowns are built to reduce the single factor that drives long-term infection risk: the crown margin. Margin precision determines whether bacteria can penetrate beneath the crown, and a gap above 100 micrometers is the threshold where bacterial ingress accelerates.
Vera Smile’s in-house 3Shape digital impression system routinely achieves margin discrepancies below 50 micrometers, narrowing the structural pathway for bacteria compared with analog impression techniques. Every crown preparation is assessed with pre-treatment X-rays and pulp vitality testing before crowning is confirmed, and if the pulp shows signs of compromise the root canal is performed first, not after an infection makes it unavoidable.
Vera Smile uses Ivoclar Vivadent bonding systems and dual-cure resin cements with lower solubility than zinc phosphate or glass ionomer alternatives, which means a longer-lasting seal at the margin. After treatment, patients receive a digital photograph of their crown margins, a hygiene protocol specific to their crown type, and a 12-month X-ray review plan, because crown placement is the beginning of the monitoring period, not the end of it.
Vera Smile holds Ministry of Health certification from the Republic of Turkey and AACD membership for its cosmetic team, and all crown work is covered by a clinical guarantee. To compare options, see our guide to dental crowns and to dental crowns cost.
FAQ
Key signs include spontaneous throbbing pain (worse at night), pain that lingers after hot or cold food, a visible bump or pimple on the gum near the crown (a fistula), a persistent bad taste or smell, and swelling of the gum around the crown base. An X-ray is the only reliable way to confirm it, because visible symptoms alone cannot distinguish a pulpal from a periodontal infection.
Treatment depends on the infection type. A pulpal infection (inside the tooth) needs root canal treatment through or after removing the crown, while a periodontal infection (in the gum) needs deep scaling, possible antibiotics, and sometimes gum surgery. Antibiotics control spread but are not a standalone cure for either type.
Yes. Secondary decay can form under a crown if the margin seal fails and bacteria penetrate between the crown and the tooth. Because it is hidden under the porcelain, it is only detectable by X-ray, so routine dental X-rays every 12 to 18 months catch secondary caries before it reaches the pulp.
The 3-3-3 rule states that a dental infection on antibiotics should show clear improvement within 3 days, should be resolved (with dental treatment) within 3 weeks, and risks chronic complications if left untreated beyond 3 months. If improvement is not evident by day 3 on antibiotics, contact your dentist rather than continuing the course and waiting.
No. A dental infection does not self-resolve. The immune system may form a chronic fistula that drains intermittently and reduces acute pain, but the bacterial source inside the tooth or gum persists. A draining fistula is not a sign the infection is clearing; it is a sign the body is managing it under pressure while damage continues.
Without treatment, a crown infection stays active indefinitely. Pain may fluctuate as the abscess fills and drains, creating a false impression of recovery, but bone destruction continues throughout. Some infections spread within days while others stay locally contained for months, and timing varies by immune response, bacterial strain, and anatomy, so there is no safe window for observation.
Not necessarily. Pain on biting is more often caused by a bite imbalance (the crown sitting too high), early pulpitis, or cracked tooth syndrome. A true infection more often causes spontaneous pain, especially at night, or heat-triggered pain that lingers. A dental examination with X-rays is the only way to confirm it, because the symptom patterns overlap too much for reliable self-diagnosis.