
Implant-supported dentures anchor a full prosthetic arch to 2-6 dental implants, eliminating the slipping and bone loss of conventional dentures. The lower jaw needs 2-4 implants; the upper jaw 4-6.
Removable overdentures (conventional) use clip or ball attachments; fixed hybrids are screw-retained permanently. Implants last a lifetime; the prosthetic arch requires replacement every 10-15 years. In the US an implant-supported denture costs $15,000-$30,000 per arch, while in Turkey a snap-on overdenture ranges from €3,000 to €8,000 per arch at the same clinical standard.
Implant-supported dentures break that cycle by anchoring the prosthesis to the bone directly with dental implants. The result is a fixed or removable denture arch that does not move, preserves the jawbone through functional loading, and lets patients eat and speak without the daily anxiety of denture adhesive.
What Are Implant-Supported Dentures?
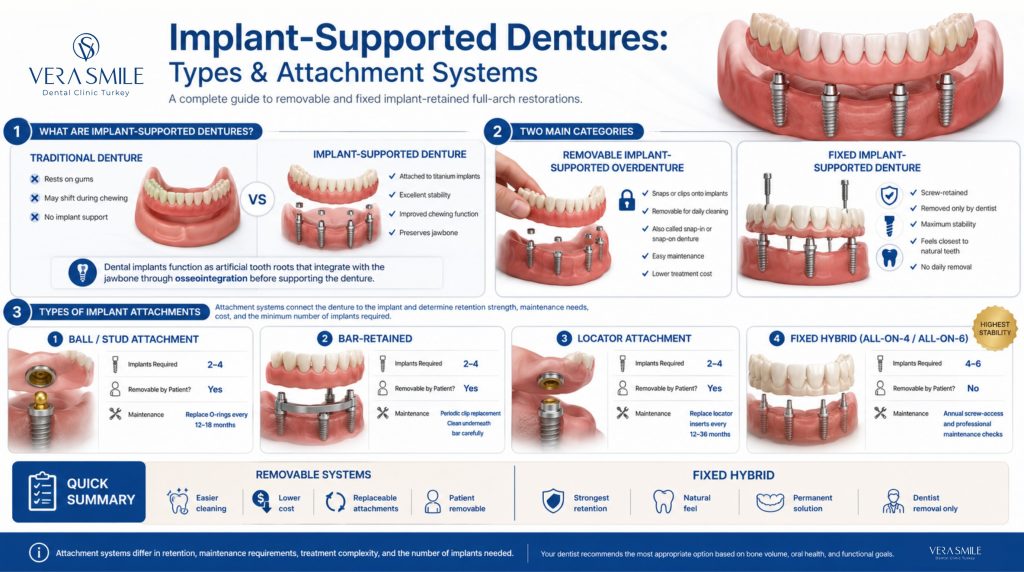
An implant-supported denture is a prosthetic arch (replacing all or most teeth in one jaw) that attaches to dental implants embedded in the jawbone rather than resting on the gum ridge. Each implant is a small threaded titanium post that acts as an artificial tooth root. Once the implants integrate with the bone (osseointegration), the dentures connect to them via one of several attachment systems.
There are two fundamental types. Removable implant-supported overdentures clip, snap, or lock onto the implants and can be removed by the patient for cleaning; these are also called snap-in or snap-on dentures. Fixed implant-supported dentures (hybrid dentures) are permanently screwed onto the implants and can only be removed by a dentist, never at home.
Terminology note: ‘snap-in dentures’, ‘snap-on dentures’, ‘implant overdenture’, ‘implant-retained dentures’, and ‘implant-supported overdenture’ all refer to the same category of removable implant denture. ‘Fixed implant dentures’ and ‘hybrid dentures’ refer to the screw-retained permanent version. The terminology varies by country and practice; the clinical distinction is always removable versus fixed.
What Is the Difference Between Snap-in and Snap-on Dentures?
There is no clinical difference between snap-in and snap-on dentures; the terms are used interchangeably in most clinical and consumer contexts. Both describe the same thing, a removable implant overdenture that physically clicks onto implant abutments rather than resting on the gum like a conventional denture. The “snap” refers to the retentive action of the attachment, whether that is a ball-and-O-ring, a locator, or a bar-and-clip system, which holds the denture firmly in place during eating and speaking but releases when the patient lifts it out to clean.
The reason two names exist is marketing and regional habit rather than any technical distinction. Some clinics and manufacturers favour “snap-on” while others say “snap-in,” and you may also see “clip-in dentures” or “implant-retained overdentures” for the identical appliance. None of these labels signals a different device, number of implants, or attachment type, so when comparing quotes it is the attachment system (ball, locator, or bar) and the number of implants that matter, not which name the clinic uses.
What Is the Difference Between Implant-Supported Dentures and All-On-4?
All-on-4 is one specific type of implant-supported denture, so the difference is one of category versus subset rather than two separate treatments. “Implant-supported dentures” is the umbrella term for any full arch anchored to implants, covering both removable overdentures (2–4 implants with ball, bar, or locator attachments that the patient takes out for cleaning) and fixed hybrid prosthetics (permanently screwed in place).
The practical differences come down to retention, function, hygiene, and cost. A removable overdenture is lower in cost, easier to clean because it lifts out, and needs fewer implants, but it restores roughly 50–70% of natural bite force and its attachment parts (O-rings or locator inserts) wear out every 12–36 months. An All-on-4 fixed hybrid restores 70–80% of bite force, never moves, and feels closest to natural teeth, but it costs more, requires cleaning in place with floss threaders and water flossers, and can only be removed by a dentist.
What Are the Types of Implant-Supported Dentures?
There are four clinically relevant types of implant-supported denture, distinguished by their attachment system. The attachment system connects the denture to the implant and determines retention strength, maintenance needs, cost, and the minimum number of implants required.
| Type | Implants Needed | Removable by Patient? | Maintenance |
|---|---|---|---|
| Ball / Stud | 2-4 | Yes | O-ring replacement every 12-18 months |
| Bar-retained | 2-4 | Yes | Clip replacement; hygiene under bar |
| Locator | 2-4 | Yes | Insert replacement every 12-36 months |
| Fixed hybrid / All-on-4 | 4-6 | No, dentist only | Screw access checks annually |
Selecting the right system depends on how you balance retention strength, maintenance commitment, and your budget. While removable options like ball, bar, or locator attachments require fewer implants and allow for straightforward at-home cleaning, a fixed hybrid prosthesis provides the highest level of stability, functioning most like your natural teeth.
What Is a Ball (Stud) Attachment Overdenture?
A ball attachment overdenture utilizes a rounded male abutment on the implant that snaps directly into a rubber O-ring housed inside the prosthesis, making it the most globally widespread system for lower jaw restoration. Requiring at least two implants for adequate retention, this option offers a highly cost-effective, easily repairable solution with a simple insertion routine that patients master quickly. However, its primary drawback is that the rubber O-rings wear down over time and must be routinely replaced every 12 to 18 months to maintain proper grip.
What Is a Bar Attachment Overdenture?
A bar attachment overdenture connects two to four implants with a customized metal bar running along the gumline, allowing the denture to securely clip into place using built-in riders. By structurally splinting the implants together, this framework evenly distributes chewing forces across the entire implant group, providing superior retention and a lower vertical profile than unsplinted systems. While exceptionally stable, it is more expensive to fabricate and requires meticulous oral hygiene, demanding the daily use of specialized interdental brushes and floss threaders to clean beneath the bar framework.
What Is a Locator Attachment Overdenture?
A locator attachment overdenture features low-profile, tissue-level abutments with a dual-retention mechanism that secures the prosthesis through both internal and peripheral engagement, maximizing stability where vertical space is limited. Widely accepted as the modern standard of care for two-implant lower overdentures, this system utilizes interchangeable nylon inserts that allow your dentist to easily customize and adjust the retention force. These color-coded inserts are much simpler to replace than traditional rubber O-rings and boast an extended lifespan of 12 to 36 months depending on individual bite force.
What Is a Fixed Hybrid (Screw-Retained) Denture?
A fixed hybrid denture is permanently anchored to four to six dental implants using titanium screws and can only be removed by a professional, offering the closest match to the function and feel of natural teeth. The most prominent example is the All-on-4 protocol, which strategically tilts the posterior implants at a 45-degree angle to maximize bone contact while safely bypassing sinus cavities and critical jaw nerves. Because this permanent prosthesis eliminates all rocking and completely eliminates upper palate coverage, patients experience fully restored biting power and a significantly enhanced sense of taste.
What Are Mini Implants for Implant-Supported Dentures?
Mini implants for implant-supported dentures are specialized dental implants with a diameter below 3.0 mm, compared with the 3.5 to 5.0 mm required for standard implants. They were specifically developed for patients with insufficient bone volume who either cannot or choose not to undergo bone grafting surgeries.
Because their smaller cross-section provides less individual structural support, mini implants require 4 to 6 implants per arch to properly stabilize a denture. They are placed using a convenient one-stage procedure with no separate abutment surgery, meaning they can often be loaded immediately with the prosthesis.
However, it is important to note that long-term clinical evidence is less robust than for standard options. While standard-diameter implants boast extensive 20-year datasets, 10-year data for mini implants remains relatively limited.
In Which Conditions Are Mini Implants Recommended?
Mini implants suit a specific subset of patients rather than the general population. They are considered in the following situations:
- Limited bone volume: Patients who lack the bone width needed for standard implants and cannot or prefer not to undergo grafting.
- Elderly or high surgical-risk patients: Those for whom a shorter, less invasive one-stage procedure is the safer choice.
- Contraindications to major grafting: Patients whose medical profile makes extensive augmentation inadvisable.
- Need for immediate stabilisation: Cases where a denture must be secured quickly with minimal healing time.
Mini implants are not a substitute for standard implants in patients who are good candidates for the standard protocol. They are a targeted solution for situations where bone volume or surgical risk rules out the conventional approach.
How Many Implants Do You Need for Implant-Supported Dentures?
Most implant-supported dentures require 2 to 6 implants per arch, specifically 2 to 4 in the lower jaw and 4 to 6 in the upper jaw. The exact number depends on bone density, jaw anatomy, the attachment system, and whether the prosthesis is removable or fixed.
The lower jaw requires 2 to 4 implants because it holds the densest bone in the mouth, classified as Type D2 or D3 on the Misch bone-quality scale. The upper jaw requires 4 to 6 implants because it features significantly lower bone density, classified as Type D3 or D4. This bone is more porous, which lowers initial implant stability, while the sinus cavities limit the depth available for posterior placement.
By evaluating specific jaw dynamics, your dental professional can create a customized treatment plan that fully restores your natural biting force and overall quality of life. Quantity of the implants should be individualized.
How Do Implant-Supported Dentures Prevent Jawbone Loss?
Implant-supported dentures prevent bone loss because the implants transmit chewing forces directly into the jawbone, restoring the stimulus that natural tooth roots once provided. When a tooth is extracted, the surrounding bone loses this biomechanical signal; osteoclastic activity outpaces osteoblastic formation, and the bone begins to resorb.
Conventional dentures accelerate this process. They load the gum ridge with compressive forces that do not simulate root-transmitted axial loading. The bone resorbs faster under the pressure zone and slower elsewhere, creating uneven ridge collapse. Dental implants reverse the stimulus deficit.
Marginal bone loss around well-maintained implants averages 0.34 mm in the first year of loading and remains near zero annually thereafter in successful cases, compared with 1-2 mm per year of ridge resorption in conventional denture wearers. (Implant-supported overdentures, a prevention of bone loss in edentulous mandibles? A 5-year follow-up study, Journal of Oral Rehabilitation, 2001)
What Is the Implant-Supported Denture Procedure?
The implant-supported denture procedure runs across multiple clinical stages spread over several months. The exact timeline depends on whether extractions, bone grafting, or sinus augmentation are needed before implant placement.
- Consultation and Digital Imaging: Dentists perform a full-mouth CBCT scan and assess your bone density to map out your prosthetic planning. During this initial visit, your specialist confirms the final treatment plan, including the exact number of implants, attachment type, and whether you require preliminary jawbone grafting.
- Tooth Extractions: The clinical team removes any remaining failing or damaged teeth to prepare your mouth for the incoming fixtures. This stage requires a healing period of 6 to 8 weeks before the surgeon can safely proceed with bone grafting or final implant placement.
- Bone Grafting: If your natural jawbone volume is inadequate, the surgeon performs socket preservation or ridge augmentation. This foundational step requires 3 to 6 months of healing to ensure a strong base for the titanium posts, though it is skipped entirely if your natural bone density is already sufficient.
- Implant Placement Surgery: The surgeon places the implants into your jawbone under local anaesthesia or sedation in a procedure lasting 60 to 120 minutes. A temporary healing denture is fitted the same day so you are never left without teeth, and your provider removes the surgical sutures 7 to 10 days later.
- Osseointegration: The titanium fixtures must fuse securely with your living bone, a vital biological process taking 3 to 4 months in the lower jaw and 4 to 6 months in the upper jaw. You will wear your temporary healing denture throughout this phase, ensuring there is no direct weight or load placed on the implants while they heal.
- Abutment Placement: Once the implants successfully fuse with the bone, you return for a short appointment. Your dentist replaces the temporary healing caps with your permanent attachment abutments, preparing the anchors for your choice of a ball, bar, or locator system.
- Prosthetic Fitting: Your clinical team takes precise dental impressions and sends them to the laboratory, where your custom-tailored denture is fabricated over 2 to 4 weeks. Once ready, you attend a fitting session to complete rigorous bite verification to ensure your alignment is perfect.
- Final Delivery and Patient Training: The dental team securely attaches your final custom denture to the integrated implants. Your clinician then provides comprehensive, hands-on training on proper insertion and removal techniques, daily cleaning routines, and long-term hygiene protocols to ensure your new smile lasts a lifetime.
The total timeline is 5-12 months from first appointment to final prosthesis. Patients who have adequate bone and need no extractions or grafting complete treatment at the shorter end of this range.
Immediate loading (same-day teeth) is possible in carefully selected patients with adequate bone density and primary implant stability, where a temporary prosthesis is attached to the implants on the day of placement. This is common for fixed All-on-4 protocols. Immediate dental implants follow specific eligibility criteria for same-day loading.
How Much Do Implant-Supported Dentures Cost?
Implant-supported denture cost varies by country, treatment complexity, implant brand, prosthetic material, and attachment type.
| Component | US Cost Range | Turkey Cost Range (Vera Smile) |
|---|---|---|
| Per implant (titanium, placed) | $1,500 – $2,500 | €350 – €600 |
| Bone graft (per site, if needed) | $500 – $3,000 | €300 – €700 |
| Overdenture prosthetic (per arch) | $3,000 – $8,000 | €1,200 – €3,000 |
| Fixed hybrid prosthetic(per arch) | $6,000 – $14,000 | €2,500 – €6,000 |
| 2-implant overdenture (lower arch, total) | $8,000 – $15,000 | €3,000 – €5,000 |
| 4-implant overdenture (per arch, total) | $15,000 – $25,000 | €5,000 – €8,000 |
| All-on-4 fixed hybrid (per arch, total) | $20,000 – $35,000 | €11,000 – €28,000 |
Insurance coverage in the US is limited. Most dental insurance plans exclude implants as a ‘cosmetic’ procedure. Some dentures cost plans to cover the prosthetic component partially. Medicare does not cover dental implants. Flexible spending accounts (FSAs) and health savings accounts (HSAs) can be used toward implant costs.
What Are the Pros and Cons of Implant-Supported Dentures vs Conventional Dentures?
Implant-supported dentures outperform conventional dentures on nearly every functional measure, but they require surgery, carry a higher upfront cost, and need periodic maintenance of their attachment components.
| Factor | Implant-Supported Dentures | Conventional Dentures |
|---|---|---|
| Stability | No slipping, rocking, or adhesive required | Shifts with jaw movement; adhesive often needed |
| Bone preservation | Implants transmit load to bone, halting resorption | Accelerates ridge resorption: up to 4 mm height loss in year one |
| Bite force | Restored to 70-80% of natural teeth | 20-30% of natural bite force |
| Chewing comfort | All foods possible, including hard and crunchy | Soft diet recommended, especially for lower dentures |
| Speech | Stable, no slippage during consonants or sustained speech | Can click or shift; affects sibilants and plosives |
| Facial support | Maintains jaw height and lip support long term | Allows progressive facial collapse over 5-20 years |
| Maintenance | O-rings replaced every 12-18 months; locators every 12-36 months | Relining required every 2-3 years as ridge shrinks |
| Prosthetic lifespan | Denture base: 10-15 years. Implants: lifetime with proper care | 5-8 years before a full replacement is needed |
| Cost | Higher upfront investment (implant placement plus prosthetic) | Lower initial cost; ongoing relining and replacement add up over time |
| Surgery required | Yes, implant placement under local anaesthesia; 3-6 month healing | No surgery required |
In short, implant-supported dentures deliver markedly better stability, bite force, and bone preservation, while conventional dentures remain the lower-cost, non-surgical option for patients who cannot undergo implant placement.
What Happens If You Don’t Get Implant-Supported Dentures when Needed?
If you delay or avoid getting implant-supported dentures when needed, you will experience a progressive condition known as facial collapse. Without dental implants to replace missing tooth roots, your underlying jawbone resorbs because it lacks functional chewing stimulation. As this bone breaks down, the lower third of your face loses its skeletal support. The vertical distance between your nose and chin shortens, your lips roll inward from a lack of backing, and your skin sags, creating a prematurely aged profile.
This structural deterioration develops gradually over years of untreated bone loss, deepening with each passing stage:
- Years 1 to 3: Your traditional denture fit deteriorates rapidly as your jaw ridge height drops, making frequent relines necessary to keep the prosthesis stable.
- Years 5 to 8: The deep folds running from your nose to the corners of your mouth intensify, lip support reduces significantly, and your lower face appears noticeably shortened.
- Year 10 onward: The loss of lower facial height becomes severe as your chin rotates upward toward your nose, causing deep jowls and a sunken appearance.
- Year 20 and beyond: Advanced jawbone atrophy sets in, which can make future implant placement impossible without undergoing extensive preliminary surgeries like bone grafting or sinus lifts.
Choosing implant-supported dentures early completely interrupts this destructive timeline. The titanium fixtures halt bone resorption at the exact moment of placement, preserving your natural facial structure and protecting your long-term health.
Who Is a Candidate for Implant-Supported Dentures?
Candidacy is determined by a combination of medical, dental, and anatomical factors. The core criteria are set out below.
- Missing most or all teeth in one or both arches: Implant-supported dentures are designed for patients who are fully or nearly edentulous in the treated arch.
- Sufficient bone volume: Minimum bone height and width is required for standard implant placement. CBCT scanning determines available bone precisely. Patients with inadequate bone can often proceed after bone grafting, which adds time and cost but restores candidacy for the majority.
- Non-smoking or willing to quit: Smoking significantly increases implant failure risk because nicotine impairs vascularisation and delays osseointegration. Most centres require smoking cessation 4-6 weeks before surgery and throughout the healing phase.
- Controlled systemic health: Well-controlled diabetes, hypertension, and osteoporosis do not automatically exclude candidacy but require careful management. Uncontrolled diabetes impairs healing; bisphosphonate therapy for osteoporosis raises the risk of medication-related osteonecrosis.
- No active oral infection: Active periodontal disease, abscesses, or untreated caries must be resolved before implant placement.
- Adequate age: Jaw growth must be complete, generally 18 or older (earlier only in exceptional clinical cases). No upper age limit applies; success rates in patients over 70 remain high when systemic health is managed.
In practice, most patients who are missing teeth in an arch qualify, and the few who lack adequate bone can become candidates after preparatory treatment.
What Happens If You Do Not Have Enough Bone?
Bone loss does not exclude you from implant treatment, as it is highly common in long-term denture wearers and routinely managed before surgery. Dentists utilize bone grafting to build up the necessary volume, while sinus lifts successfully address bone deficiencies in the back of the upper jaw. Additionally, angled fixtures like All-on-4 implants can bypass deficient zones entirely.
For cases of severe upper jaw bone loss where standard procedures are not enough, zygomatic implants offer an advanced alternative by anchoring directly into the strong cheekbone, completely eliminating the need for traditional bone grafts. Most patients who were previously told they lacked sufficient bone become excellent candidates through these pre-surgical augmentations and specialized implant techniques.
How Is the Aftercare for Implant-Supported Dentures Managed?
Aftercare centres on daily cleaning of the prosthesis and the tissue around each implant, plus a professional check every six months. The routine differs slightly between removable overdentures and fixed hybrids.
| Care Task | Removable Overdentures | Fixed Hybrid Dentures |
|---|---|---|
| Daily removal | Remove daily, ideally overnight, to rest the gum tissue | Cannot be removed at home |
| Cleaning the prosthesis | Rinse after meals; brush with a soft-bristle toothbrush and non-abrasive denture cleaner, not regular toothpaste (too abrasive for acrylic) | Clean in place; use floss threaders or super floss under the prosthetic arch |
| Soaking | Soak overnight in denture solution to keep acrylic hydrated and prevent warping | Not applicable |
| Around the implants | Clean each abutment with an interdental brush and/or floss threader to prevent peri-implantitis | Interdental brushes and water flossers (oral irrigators) reach under the fixed arch |
| Professional maintenance | Check attachment retention, replace worn O-rings or locator inserts, assess peri-implant bone radiographically (Every 6 months) | Instrument-level cleaning under the arch, annual screw torque verification, re-seal screw access holes if degraded (Every 6 months) |
Neglecting peri-implant hygiene is the leading preventable cause of late implant failure, so the cleaning routine matters as much as the surgery itself.
What Are the Common Implant-Supported Denture Problems?
Implant-supported denture problems fall into two groups, prosthetic issues affecting the denture or its attachments, and biological complications affecting the implants and surrounding tissue. Prosthetic issues are common and mostly minor; biological complications are less frequent but more serious.
- Loose or detached attachment: O-rings and locator inserts gradually lose grip as they wear with normal use.
- Denture fracture: The acrylic base or teeth can crack under heavy bite force or if the denture is dropped.
- Wear of denture teeth: Acrylic teeth lose shape and shade over 5-10 years of function.
- Sore spots: Pressure points on the gum ridge cause tenderness, most often in the first weeks of wear.
- Peri-implant mucositis: Reversible inflammation of the soft tissue around an implant, comparable to gingivitis around natural teeth.
- Peri-implantitis: Progressive, infection-driven bone loss around the implant, and the most serious biological complication of implant therapy.
- Implant failure: Loss of osseointegration during healing (early failure) or loss of bone support after years of function (late failure). Overall 10-year implant survival exceeds 95% in systematic reviews. (Implant-supported removable partial dentures compared to conventional dentures: A systematic review and meta-analysis, Clinical and Experimental Dental Research, 2022)
Most of these issues are predictable and manageable when caught at routine six-month reviews, which is why ongoing maintenance is built into treatment from day one.
How Are Denture Problems Managed?
Each problem has a defined clinical response, ranging from a quick chairside swap to targeted intervention for advanced infections.
- Loose or detached attachment: Your dentist can quickly replace worn O-rings or locator inserts during a brief chairside appointment to restore full retention.
- Denture fracture: A laboratory technician can complete a professional repair of the acrylic or framework, generally within a 24 to 48-hour window.
- Wear of denture teeth: Over time, your provider can replace individual worn teeth or fabricate an entirely new prosthetic arch to restore proper chewing alignment.
- Sore spots: Minor physical adjustments to the denture base relieve localized pressure points on your gum ridge, eliminating any rubbing or discomfort.
- Peri-implant mucositis: This early-stage inflammation is completely reversed through professional dental debridement combined with enhanced at-home oral hygiene routines.
- Peri-implantitis: This deeper condition requires early clinical debridement, antimicrobial treatment, and targeted surgical bone regeneration in severe cases to save the underlying fixture.
- Implant failure: The surgeon will remove the implant, allow the area to heal, and place a new fixture 3 to 4 months later, incorporating a bone graft first if the localized bone volume is insufficient.
Regular maintenance and prompt attention to changes ensure that most issues are resolved quickly before they escalate. Whether your restoration requires a simple component swap or a more advanced clinical correction, staying proactive with your routine checkups keeps your implant-supported system fully functional and secure.
How Do You Choose the Right Tooth Replacement Option?
The right tooth replacement depends on bone volume, budget, whether you want a removable or fixed result, and your overall health profile. Each option has a distinct clinical indication, so there is no universal best choice. Use the table below as a starting framework before discussing specifics with your dentist.
| Option | Best For | Not Suitable For |
|---|---|---|
| Traditional dentures | Patients not eligible for surgery; extreme bone loss; very limited budget | Patients who want stability, bone preservation, or full bite force |
| 2-implant overdenture | Edentulous lower jaw; adequate anterior mandibular bone; budget-conscious implant option | Upper jaw (needs more implants); patients wanting a fixed, non-removable option |
| 4-implant overdenture | Both arches; higher retention needed; bar attachment preferred | Severe posterior bone loss without augmentation |
| All-on-4 fixed hybrid | Permanent fixed teeth; full bite-force restoration; no daily removal | Active peri-implant infection; uncontrolled diabetes; insufficient bone without augmentation |
| Full mouth implants | Missing selected teeth but not an entire arch; highest aesthetic and functional outcome | Fully edentulous patients, where whole-arch replacement is cost-prohibitive |
As a rule of thumb, traditional dentures suit those who cannot have surgery, a 2-implant overdenture is the budget-conscious lower-jaw choice, a 4-implant overdenture adds retention, and an All-on-4 fixed hybrid gives fixed, full-force teeth for candidates with adequate bone.
Why Choose Vera Smile for Implant-Supported Dentures in Turkey?
Vera Smile offers full-arch implant-supported denture treatment in Turkey at a fraction of the cost of equivalent care in the UK, USA, Canada, Germany, or the Gulf region, using the same implant systems and clinical protocols. The price difference reflects lower labour costs, lower operating overheads, and a competitive private dental market; it does not reflect a difference in clinical quality at accredited centres.
Every full-arch case at Vera Smile uses CBCT-guided digital implant planning with FDA and CE-marked implant systems, including Nobel Biocare and Straumann-compatible platforms, and same-session scan-to-treatment protocols where bone allows. Each case includes a CBCT scan, digital treatment planning, implant placement under local anaesthesia or sedation, a healing denture, osseointegration monitoring, abutment placement, final prosthetic fitting, and a structured maintenance protocol from day one. Laboratory work is produced in-house or at certified partner labs to ISO-compliant specifications, and all care is governed by the Ministry of Health of the Republic of Turkey and AACD-aligned clinical standards.
FAQ
There are two types. Removable overdentures (also called snap-in or snap-on dentures) clip onto implants and can be removed by the patient for cleaning. Fixed hybrid dentures are screwed permanently to the implants and can only be removed by a dentist. Both types are stable during use; neither slips nor requires adhesive.
The titanium implants can last a lifetime with proper oral hygiene and regular maintenance, with long-term studies reporting 95%+ survival at 10 years. The prosthetic denture on top requires replacement every 10-15 years as acrylic wears and jaw anatomy changes slightly. Attachment components (O-rings, locator inserts) need replacing every 12-36 months, which is routine maintenance, not a complication.
Yes. Once osseointegration is complete and the final prosthesis is fitted, patients can eat all foods, including hard, crunchy, and chewy items that were not possible with conventional dentures. Bite force is restored to approximately 70-80% of natural teeth with a fixed hybrid, and approximately 50-70% with a well-fitted overdenture.
Yes. Implants transmit functional load to the jawbone, maintaining the biomechanical stimulus that prevents resorption. Marginal bone loss around successfully integrated implants averages 0.34 mm in the first year and approaches zero annually thereafter. Conversely, conventional dentures are associated with 1-2 mm of ridge resorption per year, causing progressive facial collapse over a decade. (Implant-supported overdentures, a prevention of bone loss in edentulous mandibles? A 5-year follow-up study, Journal of Oral Rehabilitation, 2001)
In most cases, yes, with preparation. Bone loss is extremely common in long-term denture wearers. Bone grafting restores volume in deficient sites, sinus lifts address posterior maxillary bone deficiency, and angled implants (All-on-4 protocol) bypass severely resorbed posterior zones. Patients told they ‘don’t have enough bone’ are often candidates after augmentation.