
The 6 types of dental crowns are zirconia, E.max (lithium disilicate), all-ceramic porcelain, PFM (porcelain-fused-to-metal), gold alloy, and CEREC same-day crowns. Zirconia is the most widely recommended option today because it is metal-free, exceptionally strong (900-1,200 MPa), and suitable for both front and back teeth.
There is no single “best”dental crown. The right material depends entirely on tooth position, bite force, and aesthetic priority. A crown on an upper front tooth has vastly different cosmetic and mechanical requirements than one on a lower molar, so the choice should always follow the clinical diagnosis, not clinic stock.
High-quality crowns last 10 to 25 years depending on the material and patient care. For front teeth, E.max and high-translucency zirconia give the most natural, lifelike result; for back teeth, monolithic zirconia handles the highest bite forces without fracturing.
While US prices range from $800 to $2,500 per tooth, accredited Turkey clinics offer the exact same certified materials for a fraction of that figure.
At a Glance: A dental crown is a full-coverage cap cemented over a damaged or weakened tooth. Indications include large fractures, severe decay (more than 50% of tooth structure lost), post-root canal protection, implant restoration, and cosmetic correction. Material is chosen based on tooth position, remaining tooth structure, and aesthetic requirements.
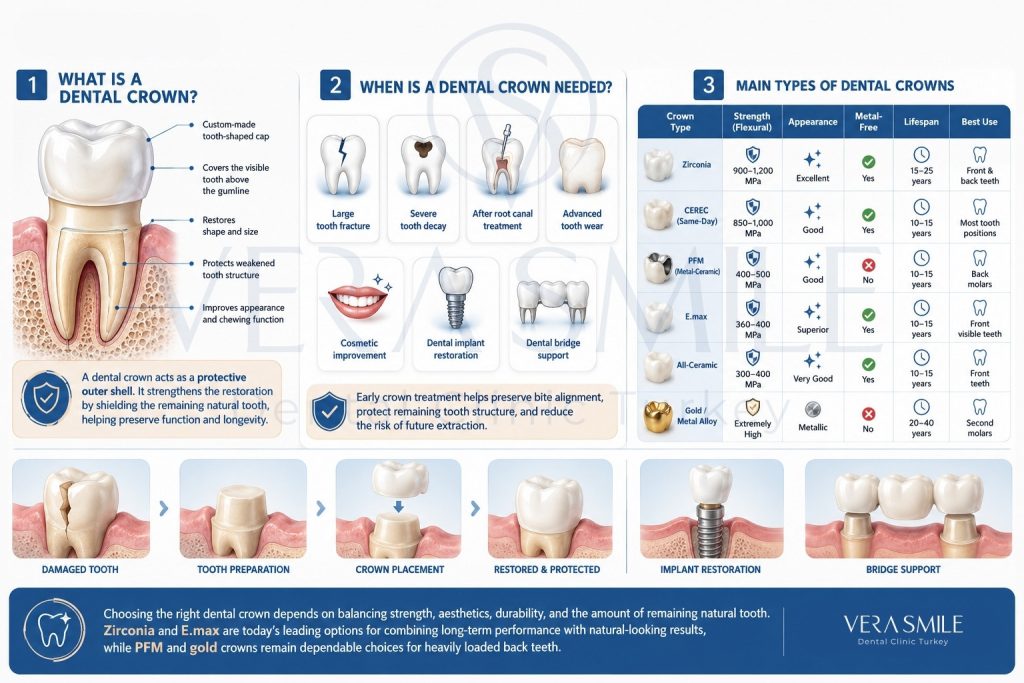
What Is a Dental Crown?
A dental crown is a custom-fitted, tooth-shaped cap that fits securely over a damaged, weakened, or cosmetically compromised tooth. Once permanently cemented, it covers the visible portion of the tooth above the gumline, restoring its shape, size, structural strength, and appearance.
A crown does not strengthen the internal tooth itself, it acts as an external shield protecting what remains of the natural structure. While a crown on a severely compromised tooth preserves chewing function, the underlying tooth anatomy still dictates the long-term prognosis. This is exactly why material choice matters; a stronger, more resilient crown becomes more critical when the remaining natural tooth structure is minimal.
When Do You Need a Dental Crown?
You need a dental crown when a tooth is damaged too extensively to be safely or predictably repaired with a standard filling. The main clinical indications are listed such as:.
- Large Structural Fractures: A crack or fracture wide enough to compromise the tooth’s structural integrity under normal chewing loads.
- Severe Cavities: Advanced decay that has destroyed more than 50% of the healthy natural tooth structure.
- Post-Root Canal Protection: Root-treated teeth become brittle and hollowed out, making them prone to fracture without a protective crown shell.
- Advanced Tooth Wear: Severe enamel erosion or loss of tooth height caused by chronic grinding (bruxism) or acid reflux.
- Cosmetic Correction: Restoring a severely discoloured, misshapen, or abnormally small tooth to create visual symmetry.
- Dental Implant Restorations: Serving as the final visible tooth that attaches to a dental implants post.
- Dental Bridge Anchors: Crowns placed on healthy teeth adjacent as a dental bridge to a gap to support a multi-unit bridge.
Addressing these vulnerabilities early lets a crown preserve bite alignment, protect the tooth root, and reduce the likelihood of a future extraction.
What Are the Main Types of Dental Crowns?
Modern restorative dentistry relies on six clinically distinct crown varieties that balance biocompatibility, mechanical durability, and cosmetic integration. Rather than utilizing a single universal material, selecting the appropriate restoration requires analyzing specific clinical variables such as structural load capacity and aesthetic priority across different zones of the mouth.
| Crown Type | Flexural Strength | Aesthetics | Metal-Free | Average Lifespan | Best Applications | Approx. US Cost |
|---|---|---|---|---|---|---|
| Zirconia | 900-1,200 MPa | Excellent | Yes | 15-25 years | Front & back teeth | $900-$1,500 |
| CEREC (Same-Day) | 850-1,000 MPa | Good | Yes | 10-15 years | Any tooth position | $1,000-$1,800 |
| PFM (Metal-Ceramic) | 400-500 MPa | Good (fades) | No | 10-15 years | Back molars | $800-$1,400 |
| E.max | 360-400 MPa | Superior | Yes | 10-15 years | Front visible teeth | $1,200-$2,000 |
| All-Ceramic | 300-400 MPa | Very good | Yes | 10-15 years | Front teeth only | $800-$1,500 |
| Gold / Metal Alloy | Extremely high | Poor (metallic) | No | 20-40 years | Second molars only | $1,000-$2,500 |
Evaluating these options based on their physical performance benchmarks, long-term survival rates, and economic profiles helps establish the ideal treatment path for each unique patient profile. Legacy materials such as PFM and gold remain durable for hidden back molars, while zirconia and E.max dominate modern practice for their combination of strength, biocompatibility, and aesthetics.
What Are Zirconia Crowns?
Zirconia (zirconium dioxide) crowns are the current clinical standard for most dental restorations. Zirconia is a metal-free ceramic with a flexural strength of 900-1,200 MPa, roughly three to four times stronger than traditional porcelain.
It is used in two formats. Monolithic (full-contour) zirconia is milled from a single solid block with no porcelain overlay, giving maximum density and fracture resistance for posterior teeth where biting pressure is highest. Layered zirconia uses a tough zirconia core topped with a glass-ceramic veneer for the aesthetics needed on visible smile-line teeth.
Zirconia Crowns: Metal-free crowns made from zirconium dioxide, with a flexural strength of 900-1,200 MPa. Monolithic zirconia suits back teeth and grinding patients; high-translucency zirconia is used for front teeth.
Who Should Get a Zirconia Crown?
Zirconia is suitable for most patients, because it is the most versatile and resilient crown material available. You are a strong candidate for a zirconia crown if you match any of the profiles below.
- Patients with Severe Bruxism: Monolithic zirconia absorbs extreme clenching and grinding forces without cracking or shearing.
- Individuals with Metal Sensitivities: Its 100% metal-free composition is safe for anyone prone to metal allergies.
- Posterior Restorations: Ideal for back molars where durability matters more than high translucency.
- Implant-Supported Restorations: Its polished surface reduces bacterial adhesion at the implant-gum junction, helping preserve bone health.
If you want a predictable, biocompatible restoration with the highest resistance to breaking under heavy chewing, zirconia is the leading choice.
What Are the Limitations of Zirconia Crowns?
Zirconia has few clinical drawbacks when designed and placed correctly, and the limitations that exist are technique-dependent rather than material-dependent. Three points are worth noting.
- Wear on Opposing Teeth: Raw zirconia is very hard (8.5 on the Mohs scale versus 5 for enamel), so an unglazed or poorly polished crown can wear down opposing natural teeth. Clinical glazing and smoothing are mandatory.
- Opacity on Front Teeth: Baseline zirconia can look slightly opaque next to translucent natural teeth, though high-translucency grades such as Katana UTML and Ivoclar ZircaCAD resolve this.
- Bonding Sensitivity: Reliable bonding requires micro-sandblasting followed by a silane coupling agent; clinics that skip these steps see higher debonding rates.
Despite these technical demands, real-world performance is strong. A 2023 systematic review published in the Journal of Dentistry compiled data from 14 clinical trials and reported a 95.5% five-year survival rate and an 89.3% ten-year survival rate for monolithic zirconia crowns, matching or exceeding legacy metal-backed options.
What Are All-Ceramic (Porcelain) Crowns?
All-ceramic crowns are fully metal-free restorations made entirely from dental glass-ceramic compounds. Their defining strength is light transmission: light passes through the porcelain and reflects off the underlying tooth like natural enamel, so a well-made all-ceramic crown is hard to distinguish from surrounding teeth.
Older feldspathic options have largely been replaced by CAD/CAM-milled blocks, and the term “all-ceramic” now refers to modern glass-ceramics or premium translucent zirconia. With a flexural strength of 300-450 MPa, these crowns handle normal biting loads on front teeth but lack the durability for back molars.
All-Ceramic Crowns: Metal-free crowns offering the highest aesthetic quality, with a flexural strength of 300-450 MPa. Best for upper front teeth where light transmission and shade matching are priorities; not recommended for posterior teeth under high bite forces.
When Are All-Ceramic Crowns the Right Choice?
All-ceramic crowns are the right choice when an invisible, highly realistic front-tooth restoration matters more than raw bite-force resistance. They suit the situations listed such as:
- Anterior Restorations: Central and lateral incisors in the smile line where maximum cosmetic blending is required.
- Critical Shade Matching: Cases where a single front tooth must match the translucency of an adjacent natural tooth.
- Hypoallergenic Dentistry: Patients who want to eliminate all metals from the oral cavity.
- Aesthetics-Sensitive Lifestyles: People frequently photographed or in public-facing roles where the smile is closely scrutinised.
In low-stress anterior positions, all-ceramic crowns deliver a life-like result that preserves the natural look of the smile.
What Is an E.max Crown?
An E.max crown is a restoration made from IPS e.max, a lithium disilicate glass-ceramic developed by Ivoclar Vivadent. It is widely regarded as the leading material for premium cosmetic dentistry and represents a major step up from traditional feldspathic porcelain.
How Is E.max Crown Different From Standard Porcelain?
The difference lies in microstructure and manufacturing. Traditional porcelain is layered and sintered manually, which can leave micro-porosities, whereas E.max is pressed under high heat or digitally milled from a single uniform block of lithium disilicate.
This produces an even crystal structure with almost no internal flaws. As a result, E.max delivers a flexural strength of 360-400 MPa, far above the 80-120 MPa of standard feldspathic porcelain, while reproducing the enamel-to-dentin translucency gradient of a real tooth so accurately that it stays undetectable under direct flash photography.
What Are PFM Crowns?
PFM stands for porcelain-fused-to-metal. A PFM crown combines an inner metal alloy coping (cobalt-chromium, nickel-chromium, or precious gold alloy) with a tooth-coloured feldspathic porcelain veneer baked on top. From the 1960s to the early 2010s this was the universal standard for dental crowns, using the metal core for strength and the porcelain layer for appearance.
PFM Crowns: Porcelain-fused-to-metal crowns have a metal alloy base with a porcelain veneer. They were the clinical standard for more than 40 years. Main drawbacks are such as porcelain chipping (15-25% over 10 years), grey gum lines as gums recede, and metal content. Zirconia has replaced PFM as the modern standard for most cases.
Are PFM Crowns Still Used?
PFM crowns are still used, but only in limited cases, and they are no longer the recommended standard for visible teeth. They remain an option for back molars where cosmetic expectations are low and the metal core offers reliable fracture resistance.
The core flaw is a material mismatch; the porcelain shell and metal core expand and contract at different rates with hot and cold foods, creating microscopic shear stress along the bond interface. Over time this causes delamination. A Cochrane Review reported that roughly 15% to 25% of PFM crowns suffer porcelain chipping or cohesive failure within 10 years.
PFM crowns also show a predictable cosmetic failure called the grey gumline problem. As gum tissue recedes by a millimetre or two over 5 to 10 years, it exposes the dark metal margin of the coping, creating a visible grey ring at the base of the tooth. This cannot be polished away and is resolved only by replacing the crown. If a provider offers a PFM crown for a visible front tooth, it is reasonable to ask why, since metal-free alternatives such as zirconia or E.max offer better cosmetics, healthier tissue, and equal or longer lifespan.
What Are Gold Crowns?
Gold crowns, more accurately called high-noble gold alloy crowns, are the oldest and most durable restorations in dentistry. Composed of 40% to 75% gold with noble metals such as platinum, palladium, or silver, a well-maintained gold crown on a back molar can last 40 years or more, outperforming every ceramic alternative on lifespan.
Who Should Consider a Gold Crown?
You should consider a gold crown if you have extreme grinding habits or need a long-lasting restoration on a hidden molar. Gold remains mechanically unmatched even though its popularity has fallen due to metal prices and demand for tooth-coloured smiles. The main candidates are listed such as:
- Extreme, Chronic Bruxism: Gold is ductile, absorbing severe clenching by burnishing slightly over time rather than cracking like ceramic.
- Second Molar Restorations: Ideal for the very back teeth, where visibility is zero but chewing forces are highest.
- Metal Allergy Management: For patients with nickel or base-metal hypersensitivity, who may experience an allergic reactions to a dental crown, high-gold noble alloy is stable, non-corrosive, and biocompatible.
- Minimal Tooth Clearance: Gold can be cast into thin, strong layers, requiring less removal of natural tooth structure, which helps patients with limited jaw opening.
Its metallic yellow appearance rules it out for front teeth, but gold remains an elite structural choice for hidden molars requiring lifetime durability.
What Is a Temporary Crown?
A temporary crown is a short-term cap placed over a freshly prepared tooth while the permanent crown is fabricated. Made from acrylic resin (PMMA) or dental composite, it is held with weak zinc-oxide cement designed for easy, non-destructive removal at the follow-up visit.
A temporary crown serves three functions such as protecting the prepared tooth from sensitivity and bacteria, maintaining spacing so adjacent teeth do not drift, and providing a functional surface and acceptable look in the interim.
How Long Does a Temporary Crown Last?
A temporary crown is designed to stay in place for about 2 to 6 weeks, which covers the standard laboratory production window. Because it is held with temporary adhesive, patients should avoid sticky, chewy, or very hard foods on that side to prevent dislodgement.
A temporary crown coming off is not an acute emergency, but leaving the prepared tooth exposed is a concern. The prepared tooth has reduced enamel and is vulnerable to bacteria, temperature shifts, and movement, so you should contact the clinic the same day to have it reattached.
What Is the Difference Between E.max and Zirconia?
Selecting between E.max and zirconia centers on navigating the fundamental engineering tradeoff between optical lifelikeness and mechanical endurance in restorative dentistry. While both materials are entirely biocompatible and metal-free, they utilize completely different crystalline structures that dictate how they handle light transmission and masticatory forces. E.max (lithium disilicate) is engineered to replicate the glass-like optical depth of natural tooth enamel, whereas zirconia (zirconium dioxide) provides a high-density crystalline framework designed to withstand extreme, repetitive structural stress.
| Factor | E.max (Lithium Disilicate) | Zirconia |
|---|---|---|
| Flexural strength | 360-400 MPa | 900-1,200 MPa |
| Best position | Visible anterior teeth | High-pressure back molars, implants |
| Bruxism suitability | Low clenching only | Severe bruxism |
| Aesthetic ceiling | Superior translucency | Excellent (high-translucency grades) |
| Primary use | Cosmetic perfection in the smile line | Structural durability |
Choose E.max for highly visible front teeth where matching neighbouring translucency is critical and the patient does not grind heavily. Choose zirconia crowns for back molars, severe bruxism, or implant crowns where the 900-1,200 MPa strength threshold is required.
What Is the Best Type of Dental Crown for Back Teeth?
The best crown for back teeth (molars and premolars) is a monolithic zirconia crown. Back teeth generate immense crushing pressure, up to 280 lbs/inch² at the molar, and monolithic zirconia absorbs these forces without fracturing or chipping while remaining metal-free. This eliminates metal allergy risk and grey gumlines, with a 10-year survival rate of 89.3%.
Because back molars are rarely visible, the slight loss of translucency compared with E.max is irrelevant here. Zirconia is also more cost-effective than gold in most markets. The one exception is severe, unmanaged bruxism in patients who have repeatedly cracked ceramic restorations; for them, a ductile gold alloy crown on a second molar remains the best alternative, since its wear rate mirrors natural enamel and protects opposing teeth.
What Is the Best Type of Dental Crown for Front Teeth?
The best crown for front teeth (central incisors, lateral incisors, and canines) is either an E.max or a high-translucency zirconia crown, decided case by case. E.max is the first choice when maximum cosmetic perfection is the goal and the patient does not grind, because a ceramist can layer it to mirror the depth, texture, and light transmission of a real tooth.
When a front-tooth case needs both beauty and added strength, such as a light clenching habit or an implant-supported anterior crown, premium high-translucency zirconia grades like Katana UTML or Ivoclar ZircaCAD are preferred. They offer near-E.max cosmetics with a robust zirconia core. Legacy PFM, standard opaque monolithic zirconia, and gold are avoided for front teeth due to grey gumlines, opacity, or obvious metallic appearance.
How Much Does Each Type of Dental Crown Cost?
Dental crown pricing varies by material, clinic location, laboratory, and provider expertise. In the United States, general practices price crowns between $800 and $2,500 per tooth, with many insurance plans covering up to 50% after the annual deductible.
| Crown Material | Average US Cost Range (Per Tooth) | Insurance Coverage Notes |
|---|---|---|
| All-Ceramic / Porcelain | $800 – $1,500 | Often covered at 50% if medically necessary |
| PFM (Metal-Ceramic) | $800 – $1,400 | Widely approved due to legacy classification |
| Zirconia | $900 – $1,500 | Standard coverage; accepted as the modern norm |
| CEREC Same-Day | $1,000 – $1,800 | Covered similarly to lab crowns; some clinics add a tech fee |
| E.max (Lithium Disilicate) | $1,200 – $2,000 | Higher out-of-pocket due to premium lab fabrication |
| Gold / Metal Alloy | $1,000 – $2,500 | Variable; tied to market gold rates |
Choosing a specialist prosthodontist can raise these rates by 20% to 40%. In Turkey, accredited clinics provide the same certified zirconia and E.max materials at lower cost; most patients choose to come to Turkey due to dental crown cost in Turkey.
How Long Does Each Type of Dental Crown Last?
While a dental crown is designed to be a long-term structural restoration, its actual survival rate is dictated by a dynamic interplay between material science, patient-specific bite forces, and meticulous marginal hygiene. Rather than relying on a universal estimate, evaluating longevity requires looking at how different compounds withstand the daily mechanical stress of mastication. Long-term clinical data provides a clear benchmark for expected lifespans and primary failure modes across each major restoration category.
| Crown Material | Average Lifespan | Key Clinical Data and Primary Failure Modes |
|---|---|---|
| Gold / Metal Alloy | 20-40+ years | Most durable; lowest fracture rate in clinical history |
| Zirconia (Monolithic) | 15-25 years | 95.5% survival at 5 years; 89.3% at 10 years (Journal of Dentistry) |
| E.max (Lithium Disilicate) | 10-15 years | 93% survival at 10 years in low-force anterior positions |
| CEREC Same-Day | 10-15 years | Clinically equivalent to lab crowns of the same block |
| PFM (Metal-Ceramic) | 10-15 years | Metal core lasts; 15-25% chip within 10 years |
| All-Ceramic / Feldspathic | 10-15 years | Strong aesthetics; higher failure under heavy loads |
Across all materials, unmanaged grinding is the leading cause of premature failure and can cut a crown’s lifespan by 40% to 60%, so a custom nightguard is essential. The crown itself does not decay, but the natural tooth at the cement margin remains vulnerable, making daily flossing critical to preventing marginal cavities.
Frequently Asked Questions
No, dental crowns cannot be whitened. Crown materials do not respond to bleaching agents, so the shade is fixed at fabrication. If a crown no longer matches whitened natural teeth, it must be replaced to change its colour.
No, the procedure itself is not painful because it is performed under local anaesthesia. Mild sensitivity to temperature or pressure for a few days afterward is normal and usually settles on its own.
Yes, many crowns are placed without a root canal. A root canal treatment is only needed if the tooth’s nerve is infected or irreversibly inflamed; a tooth that is structurally damaged but healthy can be crowned directly.
A crown covers the entire tooth above the gumline, while a dental veneers covers only the front surface. Crowns are used for structural damage; veneers are used for cosmetic changes on otherwise sound teeth.