
Allergic reactions to dental crowns are uncommon but well documented, with the most frequent triggers being base-metal alloys containing nickel, chromium, cobalt, or beryllium, found in some porcelain-fused-to-metal (PFM) and non-precious cast crowns. Reactions are Type IV delayed hypersensitivity (contact allergy), not immediate anaphylaxis. Symptoms include gum redness or swelling at the crown margin, burning or metallic taste, mouth ulcers near the crown, cheek or lip dermatitis touching the crown, and rarely lichenoid lesions.
Diagnosis is by dermatology patch testing, not by clinical inspection alone. Treatment is replacement of the crown with a hypoallergenic material: monolithic zirconia, lithium disilicate (E.max), all-ceramic feldspathic porcelain, or high-noble gold. True allergy to zirconia or lithium disilicate is exceptionally rare.
What Are Allergic Reactions to Dental Crowns?
Allergic reactions to dental crowns are immune-mediated responses to a component released from the crown material, most often a metal ion from a base-metal alloy. The crown itself does not cause the allergy; the released ion does. Two immunological categories apply. The first and by far most common is Type IV (delayed) hypersensitivity, a T-cell-mediated contact allergy that develops hours to days after exposure and accounts for nearly all reactions seen with dental metals. The second is Type I (immediate) hypersensitivity, an IgE-mediated response that appears within minutes and is extremely rare with dental crown materials. Most symptoms are local rather than systemic, because the contact between the gum, oral mucosa, or lip and the released metal ion is what drives the reaction.
Why Do Allergic Reactions Occur to Dental Crowns?
Allergic reactions to dental crowns occur because the immune system reacts to metal ions released from the crown, almost always from a base-metal alloy rather than from the ceramic or precious-metal portion. The trigger is the released ion, not the crown as a solid object.
Base-metal alloys such as nickel-chromium and cobalt-chromium shed small quantities of ions into saliva and gum tissue, and nickel is the single most common dental contact allergen, followed by chromium, cobalt, and beryllium. Porcelain-fused-to-metal crowns carry the metal in their substructure, so the risk comes from the framework rather than the porcelain surface. Whether a given patient reacts depends on individual immune sensitisation, which can be primed by earlier metal contact elsewhere on the body, and on how much ion is released, which rises with corrosion, mixed metals in the same arch, and gum recession that exposes more of the alloy.
Because the cause is the alloy rather than the crown design, the most direct way to remove the risk is to remove the metal. Patients with confirmed nickel or chromium sensitivity can avoid the trigger entirely by choosing an all-ceramic or high-noble crown.
How Common Are Dental Crown Allergies?
True allergic reactions to dental crowns are uncommon, affecting fewer than 1% of crown wearers, even though skin-level metal sensitivity is far more widespread in the general population. The oral mucosa is more tolerant than skin, so a positive skin reaction does not reliably translate into oral symptoms. The table below sets out how frequency differs by group and material.
| Group or material | Approximate frequency | Notes |
|---|---|---|
| Nickel sensitivity, women (general population) | About 10 to 15% skin reactivity | Oral expression is far less frequent than skin reactivity |
| Nickel sensitivity, men (general population) | About 1 to 3% skin reactivity | Same gap between skin reactivity and oral symptoms |
| Symptomatic dental crown allergy | Fewer than 1% of crown wearers | Clinically meaningful reaction to a crown material |
| All-ceramic crowns (zirconia, lithium disilicate, feldspathic) | Exceptionally rare | Only isolated case reports in the literature |
| High-noble gold alloy | Very rare | Gold contact allergy exists, but oral relevance is limited |
A documented skin allergy to nickel does not mean a patient is allergic to a dental crown. Many people with nickel sensitivity tolerate base-metal restorations because the oral environment differs from skin, and patch testing is the only reliable way to confirm clinical relevance.
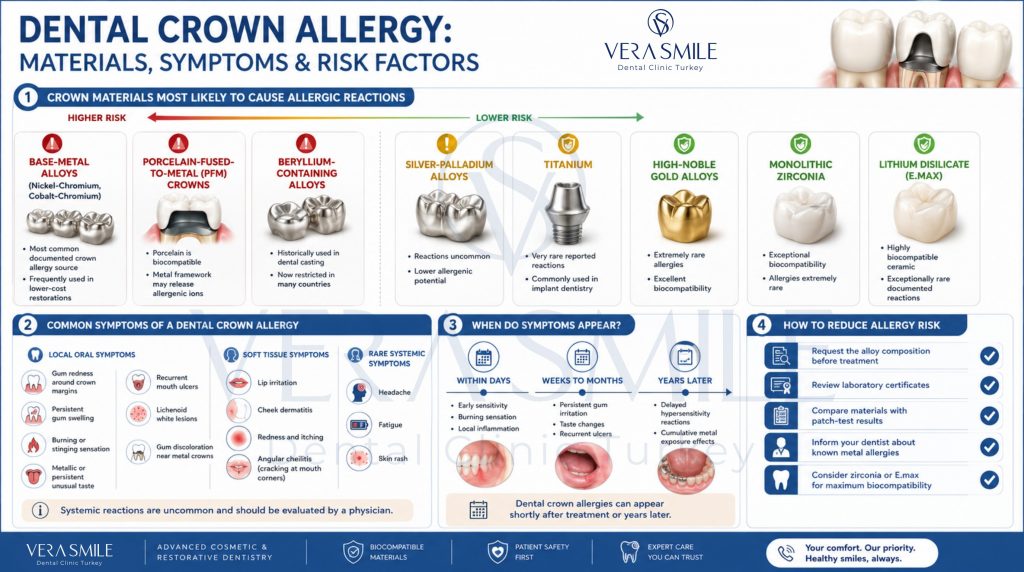
Which Crown Materials Cause Allergic Reactions Most Often?
Base-metal alloys containing nickel, chromium, cobalt, or beryllium cause most documented allergic reactions to dental crowns. Porcelain-fused-to-metal (PFM) crowns and base-metal cast crowns are the most frequently implicated categories.
- Base-metal alloys (Ni-Cr, Co-Cr): Most common offenders, used in low-cost PFM crowns and some full-cast restorations.
- Porcelain-fused-to-metal (PFM) crowns: The metal substructure may release ions, while the porcelain layer itself is biocompatible.
- Beryllium-containing alloys: Once common in dental casting, now restricted in many countries due to allergenicity and occupational risk in dental labs.
- Silver-palladium alloys: Lower allergenic potential than base-metal alloys; reactions exist but are rare.
- Amalgam and amalgam contact: Not a crown material, but relevant when adjacent restorations are present; mercury allergy is rare and contested.
- Titanium: Used in implant abutments; allergic reactions are very rare and remain debated in the literature.
- High-noble gold alloys: Very rarely allergenic; reactions are isolated case reports.
- Monolithic zirconia and lithium disilicate (E.max): Considered biocompatible, with exceptionally rare documented allergies.
If allergy is a concern, ask for the alloy composition of any proposed metal-containing crown. Lab certificates declare the exact percentages of each metal, which lets the patient cross-check against a known sensitivity list from patch testing.
What Are the Symptoms of a Dental Crown Allergy?
The most common symptoms of a dental crown allergy are localised gum redness or swelling at the crown margin, burning or metallic taste, mouth ulcers near the crown, lip or cheek dermatitis where soft tissue contacts the crown, and lichenoid lesions on adjacent mucosa. Systemic reactions are very rare.
- Gum redness and swelling at the crown margin: Persistent inflammation localized to one or two crowns, not responding to dental hygiene improvement.
- Burning or stinging sensation: Constant or intermittent oral burning, particularly in the area of the crown.
- Metallic or persistent unusual taste: A sustained taste change without identifiable food cause.
- Mouth ulcers or aphthous-like sores: Recurrent ulcers in tissue that contacts the crown.
- Lip or cheek dermatitis: Red, scaly, or itchy patches on the lip or inner cheek that touches the crown.
- Lichenoid lesions: Whitish, lace-like patterns on the mucosa adjacent to the crown.
- Angular cheilitis: Cracking or inflammation at the corners of the mouth, particularly when multiple metal restorations are present.
- Gum hyperpigmentation: Darkening of the gum margin around PFM crowns from metal ion deposition (cosmetic rather than allergic, but often confused with it).
- Generalised symptoms: Headache, fatigue, or skin rash distant from the mouth; rare, often unrelated, and best assessed by a physician rather than assumed to be crown-driven.
Symptom timing varies. Reactions can develop within days of crown placement or only after years of cumulative exposure.
How Are Dental Crown Allergies Diagnosed?
Dental crown allergy is diagnosed by combining clinical history, exclusion of infection or mechanical irritation, and dermatology patch testing with a dental-specific allergen series. Clinical signs alone cannot confirm an allergy because gingivitis, infection, and lichenoid drug reactions look similar.
- Reviewing Medical and Clinical History : Evaluating the exact timing of when symptoms started relative to the crown placement, checking for a history of skin metal allergies or jewelry reactions, and reviewing prior dental work.
- Conducting a Clinical Examination: Inspecting the soft tissue directly surrounding the crown, evaluating the integrity of the gum margins, and identifying whether the issue is simply caused by physical friction (mechanical irritation).
- Excluding Underling Infection: Taking X-rays and performing pulp viability testing to rule out an infection beneath the crown, which can mimic allergy symptoms.
- Disclosing the Crown Material: Retrieving the laboratory certificate or original fabrication records to identify the exact metal alloy composition used in the crown.
- Performing Dermatology Patch Testing: Administering the “gold standard” test where a panel of dental metals is applied to the skin (usually the back) and evaluated at 48 and 96 hours to detect delayed allergic reactions.
- Conducting an Oral Mucosal Biopsy: If lichenoid (white, lace-like) lesions are present, a biopsy is performed to distinguish a localized contact reaction from a systemic condition like oral lichen planus.
- Diagnostic Removal (Last Resort): If the diagnosis remains unconfirmed, the suspected crown is removed and replaced with a known biocompatible temporary material, while tracking whether symptoms subside.
Because several of these conditions can be present at once, diagnosis works as a process of elimination rather than a single test. Infection and mechanical irritation are ruled out first, and a confirmed allergy rests on a positive patch test that matches the metal present in the crown. Onset timing and the location of the soft-tissue changes guide which steps carry the most weight in each case.
Clinical Note: Self-diagnosis is unreliable. Many patients labelled as “allergic” to dental crowns have undiagnosed gingivitis, an infection, or mechanical irritation. The diagnostic step that matters most is patch testing, performed by a dermatologist using a dental allergen series.
What Is the Difference Between an Allergic Reaction and a Dental Crown Infection?
An allergic reaction to a dental crown is immune-driven and shows persistent localised soft-tissue changes without bone loss or systemic infection signs, while a dental crown infection is bacterial and shows pain, pus, swelling, a gum pimple, or X-ray bone changes. The two conditions overlap clinically and can coexist.
| Feature | Allergic reaction | Infection |
|---|---|---|
| Onset | Gradual, sometimes years after placement | Often weeks to months, with progression |
| Pain | Mild burning or none | Throbbing, sharp, often severe |
| Swelling | Subtle, localised, persistent | Pronounced, may spread to face |
| Pus or sinus tract | Absent | Often present |
| X-ray findings | Normal bone | Bone loss or periapical lesion |
| Response to antibiotics | None | Temporary improvement |
| Patch test result | Positive to specific metal | Negative or irrelevant |
| Tissue appearance | Lichenoid or contact dermatitis pattern | Red, swollen, possibly draining |
Distinguishing between a dental infection and an allergy is critical because an untreated infection can cause severe damage like bone loss or abscesses, making it the top priority to rule out first using X-rays and pulp testing.
An allergy is only considered after infection and mechanical irritation are excluded, and is then confirmed via patch testing. If both problems coexist, the infection is always treated first. Patients must avoid self-treating, as using steroids for a suspected allergy will dangerously worsen an unrecognized infection.
Which Dental Crown Materials Are Hypoallergenic?
The most reliable hypoallergenic dental crown materials are monolithic zirconia, lithium disilicate (E.max), all-ceramic feldspathic porcelain, and high-noble gold alloys, all of which show very low rates of documented allergy in the published literature.
- Monolithic zirconia: Composed of yttria-stabilised zirconium oxide, this highly biocompatible material carries an exceptionally rare risk of documented allergy and serves as the most common metal-free choice for high-strength posterior crowns.
- Lithium disilicate (E.max): This biocompatible, pressed glass-ceramic delivers a flexural strength of 360 to 400 MPa and is utilized for aesthetic crowns in areas where biting stress remains moderate.
- All-ceramic feldspathic porcelain: Primarily chosen for anterior aesthetic crowns, this glass-based ceramic offers excellent biocompatibility to ensure a safe and natural-looking restoration.
- High-noble gold alloy: Containing at least 60% gold alongside other noble metals, this alloy provides low allergenic potential, is exceptionally well tolerated by gum tissue, and is used to create durable posterior crowns with gum-friendly margins.
- Layered zirconia: Designed with a zirconia core and a porcelain overlay, this biocompatible option is ideal for achieving superior, natural aesthetics without compromising on a strong core.
The shift from base-metal alloys to monolithic zirconia and lithium disilicate has lowered the incidence of dental crown allergy in current practice. For patients with confirmed nickel or chromium sensitivity, an all-ceramic crown removes the trigger entirely while matching the strength and lifespan of older metal-containing options.
Can a Dental Crown Allergy Develop Over Time?
Yes. A dental crown allergy can develop years after the crown was placed, because Type IV hypersensitivity requires repeated immune exposure before it becomes clinically symptomatic. A patient who tolerated a base-metal crown for a decade can still develop symptoms later.
Several changes can push a tolerated crown toward a symptomatic reaction. Gradual ion release increases as the cement and metal surface weather over time, while new skin exposure to nickel or cobalt from jewellery, watches, or mobile phones can sensitise the immune system independently of the mouth. Pregnancy or hormonal change can alter immune reactivity, and the introduction of a second metal restoration raises the total metal load and can create galvanic effects between dissimilar metals. Periodontal recession then exposes more of the metal substructure to gum tissue, increasing direct contact with the alloy.
The timing of symptom onset is itself a diagnostic clue. A reaction that begins long after placement still warrants investigation rather than dismissal, because removing the trigger remains the only definitive resolution.
How Are Allergic Reactions to Crowns Treated?
Treatment of an allergic reaction to a dental crown is replacement of the implicated crown with a confirmed biocompatible material, combined with management of any persistent oral inflammation while the diagnosis and replacement are arranged. Antihistamines are not curative and play only a supportive role.
- Confirm the diagnosis: Patch testing identifies the specific metal allergen.
- Identify the source crown: Lab records, X-rays, and direct material analysis where needed.
- Replace with a hypoallergenic material: Monolithic zirconia, lithium disilicate, all-ceramic feldspathic, or high-noble gold.
- Manage soft-tissue inflammation: Saline rinses, soft-tissue care, and short-term topical corticosteroids in selected cases under specialist supervision.
- Address coexisting infection or gingivitis: Often present alongside the allergic component and treated separately.
- Re-evaluate adjacent restorations: Where multiple metal-containing restorations are present, sequence replacement based on symptom contribution and budget.
- Follow up post-replacement: Symptoms resolve within weeks once the trigger is removed.
Antihistamines reduce immediate-type reactions but have limited effect on Type IV delayed hypersensitivity, which is what dental crown allergies most often are. Removing the trigger is the only definitive treatment.
How Can Patients Prevent Allergic Reactions to Dental Crowns?
Patients can lower the risk of allergic reactions to dental crowns by choosing metal-free materials when feasible, disclosing all known allergies, requesting alloy composition certificates, and considering patch testing where there is a strong history of metal sensitivity.
- Disclose known metal allergies: Tell the dental team about any reactions to jewellery, watches, or clothing buttons at the consultation.
- Request alloy composition disclosure: Ask for the percentage of nickel, chromium, and cobalt in any proposed metal-containing crown.
- Choose metal-free materials for higher-risk cases: Select monolithic zirconia, lithium disilicate, or all-ceramic where allergy concern is meaningful.
- Consider patch testing in advance: Arrange testing beforehand where there is a documented history of severe contact dermatitis to metals.
- Avoid mixing different metals in the same arch: Reduce galvanic effects, which can increase ion release.
- Maintain six-month professional cleanings: Allow any early gum reaction at a crown margin to be detected.
- Review existing restorations after life changes: Reassess if new oral symptoms appear after an event such as pregnancy or a new occupation involving metal contact.
Transparent communication with your dental team and choosing the right material beforehand will save you from an uncomfortable allergy ordeal later on. Remember, the best surprise in oral health is no surprise at all-so take precautions early and don’t leave your smile to chance.
Why Choose Vera Smile for Metal-Free Dental Crown Treatment?
Vera Smile is a dental clinic in Istanbul and part of Vera Clinic Medical Center, offering metal-free crown options for patients who want to avoid base-metal alloys. The clinic works across the full range of dental crowns, so the material is matched to each case rather than fixed in advance, and a metal-free plan is selected when allergy is a concern.
For allergy-conscious patients, Vera Smile provides:
- Metal-free crown materials: Monolithic zirconia, lithium disilicate (E.max), and all-ceramic porcelain crowns are available for patients with confirmed or suspected metal sensitivity.
- Digital intraoral scanning: 3D scans replace putty impressions for accurate, comfortable measurement of the prepared tooth.
- CAD/CAM and in-house milling: Crowns are designed and milled digitally, which supports precise margins and, in suitable cases, same-day placement.
- Digital shade matching: Shade-matching devices select crown colour against the natural teeth and surrounding lighting.
- Digital Smile Design: Anterior cases are planned so aesthetics and material choice are decided together.
- Clinician-led planning: Treatment is led by the clinical team, including Dr. Mümin Manassra, DDS, with material options explained before any tooth preparation begins.
Patients with a known or suspected metal allergy receive a treatment plan that records the chosen material, so the restoration is matched to their needs. A free consultation is available to review the options before any work starts at Vera Smile.
FAQ
True allergy to zirconia is extremely rare, with only isolated case reports in the published literature. Most reactions reported around zirconia crowns turn out to be cement-related, plaque-related, or due to a coexisting condition. Patch testing remains the diagnostic standard if the suspicion is real.
Reactions can appear within days, within weeks, or after years of tolerance, because Type IV hypersensitivity requires repeated immune exposure to become symptomatic. Early reactions in the first month and very late reactions years after placement are both well documented.
No. Greyish or dark discolouration of the gum margin around a porcelain-fused-to-metal crown is most often metal-ion staining of the tissue, not an allergic reaction. The staining is cosmetic, while a true allergic reaction includes inflammation, ulceration, or lichenoid changes.
Yes. Dermatology patch testing with a dental allergen series can be arranged before crown fabrication when there is a strong history of metal sensitivity. Results guide the material choice and are particularly relevant for patients with prior severe contact dermatitis.
Yes. Monolithic zirconia crowns commonly last 15 or more years, and lithium disilicate crowns commonly last 10 to 15 years. Their lifespan is comparable to or longer than older PFM crowns, and they remove the allergenic metal load entirely.
Schedule a dental assessment to exclude infection or mechanical irritation first, since both look similar to allergy. If allergy is suspected after that step, ask for a referral to a dermatologist for patch testing. Do not self-prescribe steroids or stop other medications without supervision.