
Dental veneers come in seven recognised types: porcelain (feldspathic), lithium disilicate (E.max), composite, zirconia, no-prep porcelain (including Lumineers), palatal veneers, and snap-on veneers. The first five are the mainstream cosmetic options; palatal and snap-on are specialty or non-clinical categories. They differ across three measurable variables: flexural strength, the depth of tooth preparation required, and long-term shade stability. Porcelain feldspathic veneers remain the reference for natural translucency and last 10 to 15 years. Lithium disilicate (E.max) combines high strength (360–400 MPa) with thin preparation and lasts 12 to 20 years. Composite veneers cost the least but wear in 5 to 7 years. Zirconia is reserved for high-load cases where strength outweighs translucency. No-prep porcelain conserves enamel for light shade and shape changes. Palatal veneers treat lingual erosion on upper front teeth, and snap-on veneers are temporary removable appliances. The right type depends on aesthetic priority, durability, preparation tolerance, and budget.
What Are the Main Types of Dental Veneers?
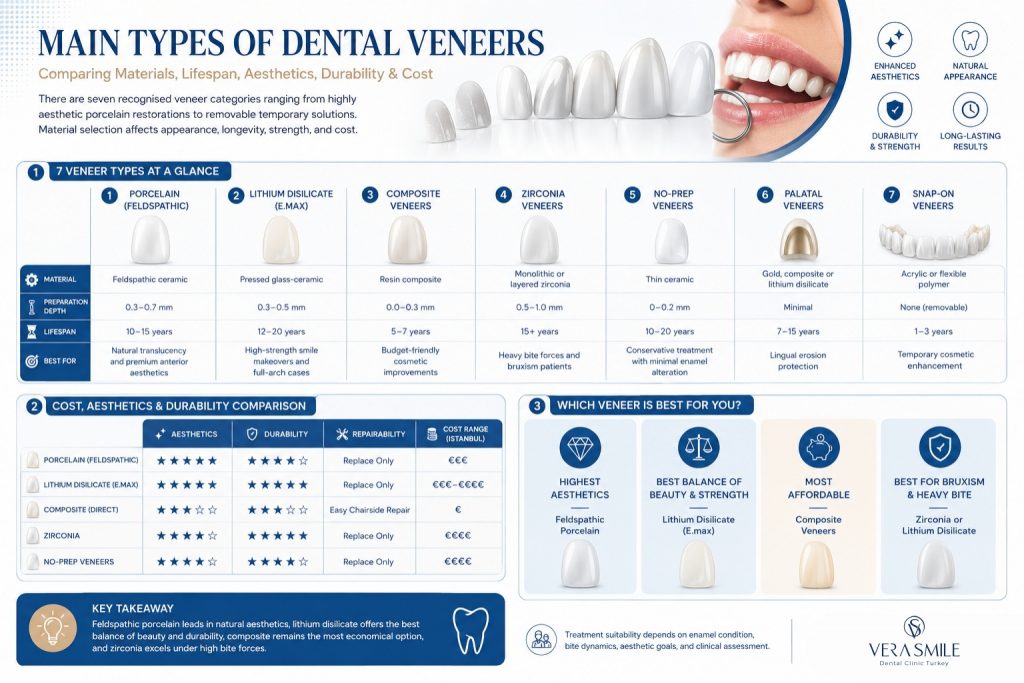
There are seven recognised types of dental veneers, split into permanent cosmetic restorations and specialty or non-clinical options. The table below summarises material, preparation depth, lifespan, and best-use case for each type.
| Veneer type | Material | Preparation depth | Average lifespan | Best clinical use |
|---|---|---|---|---|
| Porcelain (feldspathic) | Feldspathic ceramic | 0.3–0.7 mm | 10–15 years | Natural translucency for anterior aesthetics |
| Lithium disilicate (E.max) | Pressed glass-ceramic | 0.3–0.5 mm | 12–20 years | High-strength aesthetic cases, full-arch smile design |
| Composite (direct/indirect) | Resin composite | 0.0–0.3 mm | 5–7 years | Budget cases, single tooth, minor corrections |
| Zirconia | Monolithic or layered zirconia | 0.5–1.0 mm | 15+ years | High occlusal load, posterior visibility, bruxers |
| No-prep porcelain (including Lumineers) | Thin feldspathic or pressed ceramic | 0–0.2 mm | 10–20 years | Conservative cases, light shade change, narrow teeth |
| Palatal veneers | Gold alloy, composite, or lithium disilicate | Erosion-driven, minimal | 7–15 years | Lingual erosion on upper anteriors |
| Snap-on veneers | Acrylic or flexible polymer | None (removable) | 1–3 years (non-clinical) | Temporary aesthetic mask, not a clinical restoration |
The first five rows cover virtually every cosmetic veneer decision. The last two, palatal and snap-on, are specialty or non-clinical categories included for completeness.
What Are Porcelain Veneers?
Porcelain veneers are thin shells of feldspathic ceramic bonded to the front surface of the tooth to correct shape, shade, or alignment. Feldspathic porcelain has been the reference material in cosmetic dentistry for more than four decades because it reproduces the optical translucency of natural enamel more closely than any other ceramic.
Among all veneer ceramics, feldspathic porcelain offers the highest translucency, producing a natural light scatter at the incisal edge. Its flexural strength of 60 to 90 MPa is lower than lithium disilicate or zirconia, which is why enamel bonding is essential for survival. Preparation depth runs from 0.3 to 0.7 mm, leaving most of the enamel intact, and the restorations last 10 to 15 years on average, with documented cases beyond 20 years. Porcelain veneers suit anterior smile design where natural translucency is the priority and bite forces are normal. Because feldspathic porcelain is highly technique-sensitive, layered veneers built by an experienced ceramist give the most lifelike result but need longer lab time than pressed ceramics.
What Are Lithium Disilicate (E.max) Veneers?
Lithium disilicate veneers, marketed as IPS e.max by Ivoclar, are pressed glass-ceramic restorations with two to three times the flexural strength of feldspathic porcelain. They are the most widely used aesthetic veneer in modern digital workflows because they balance strength, translucency, and thin preparation.
With a flexural strength of 360 to 400 MPa, lithium disilicate tolerates thinner preparations without fracture risk, and its preparation depth of 0.3 to 0.5 mm is often the most conservative achievable for a strong ceramic. Aesthetically it offers high translucency, sitting slightly below feldspathic porcelain. The material lasts 12 to 20 years, with 5-year survival rates of 95% or higher in clinical investigations. Pressed from a digital design or wax pattern, it is fully compatible with CAD/CAM and Digital Smile Design protocols. Lithium disilicate is the only veneer ceramic that combines high strength with thin enamel-conserving preparation, which is why E.max is the standard choice for most full-arch aesthetic cases.
What Are Composite Veneers?
Composite veneers are tooth-coloured resin restorations placed directly on the tooth in a single visit or fabricated indirectly in the lab and bonded as a unit. They are the most affordable veneer category and the only one repairable chairside.
Composite veneers come in two clinical sub-types defined by where they are fabricated. Direct composite veneers are built layer by layer on the tooth in a single appointment, then sculpted and polished, with no lab work or temporaries, while indirect composite veneers are fabricated on a model in the lab and bonded as finished units, much like a ceramic veneer workflow. Across both sub-types, the resin reaches a hardness of around 80 to 100 VHN, well below porcelain at 460 or more VHN. Aesthetics are acceptable at placement, though the resin matrix loses gloss and absorbs pigment within 24 months. The restorations last 5 to 7 years on average, with annual failure rates of 3% to 5%, and chips or surface stains can be polished or repaired in a single chairside visit. Cost is the lowest of all veneer types, often half the price of porcelain. Composite veneers suit single-tooth corrections, budget cases, or a reversible trial before committing to ceramic, but they are not the right choice for full-arch makeovers where long-term shade stability matters.
What Are Zirconia Veneers?
Zirconia veneers are restorations milled from monolithic or layered zirconia, used where strength outweighs maximum translucency. They are the strongest veneer ceramic, with flexural strength above 900 MPa for monolithic zirconia.
Zirconia delivers the highest strength of any veneer ceramic, which makes it suitable for severe bruxers and posterior visible teeth. Modern multi-layered zirconia approaches lithium disilicate in translucency but stays slightly more opaque. Preparation runs from 0.5 to 1.0 mm, slightly deeper than E.max, and reliable adhesion requires zirconia-specific primers and adhesive cements. Bonded correctly, zirconia veneers last 15 years or more, comparable to or beyond lithium disilicate. They are used selectively; for most anterior cosmetic cases, lithium disilicate gives a better aesthetic outcome.
What Are No-Prep Veneers and Lumineers?
No-prep veneers are ultra-thin ceramic shells, 0.2 to 0.3 mm thick, bonded directly to the tooth surface without enamel removal. Lumineers is the most recognised brand in this category, manufactured by Den-Mat from a specific porcelain.
Because preparation is minimal or absent, no-prep veneers preserve the natural enamel and remain reversible in most cases, and at 0.2 to 0.3 mm they are roughly the thickness of a contact lens. They suit patients with small, narrow, or short teeth that benefit from slight bulking out, and patients seeking a light shade change. Their main limitation is that they cannot mask very dark teeth, severe rotations, or large alignment changes, because there is no enamel reduction to make room for the restoration. Bonded to enamel, they last 10 to 20 years, comparable to standard porcelain. A no-prep case still requires a digital mock-up to confirm that the added bulk will not produce over-contoured teeth, since no preparation does not mean no planning.
What Are Palatal Veneers and Snap-On Veneers?
Palatal veneers cover the lingual surface of upper front teeth eroded by acid reflux, bulimia, or dietary acid, while snap-on veneers are non-clinical removable acrylic appliances that clip over the natural teeth for a temporary effect. The two categories serve different purposes and are grouped here as specialty and non-clinical options.
Palatal veneers are made from gold alloy, composite, or lithium disilicate, depending on the depth of erosion and the bite, and they restore lost lingual tooth structure to stop further wear while keeping the front surface natural. Depending on material and bite, they last 7 to 15 years. Snap-on veneers, by contrast, are fabricated from acrylic or flexible polymer using a single impression or digital scan and deliver a temporary cosmetic effect for weddings, photoshoots, or trial smile previews. Because they are not bonded and not a clinical restoration, they may interfere with speech and eating, and they are included here for completeness rather than as a substitute for bonded ceramic or composite veneers.
Which Type of Veneer Lasts the Longest?
Lithium disilicate (E.max) veneers last the longest in everyday clinical conditions, with documented survival of 12 to 20 years and 5-year survival rates above 95%. The four mainstream materials rank as follows by documented lifespan.
- Lithium disilicate (E.max): 12 to 20 years, with 5-year survival rates above 95%, the longest in everyday conditions.
- Zirconia: 15 years or more, matching or exceeding lithium disilicate in heavy-load cases.
- Porcelain (feldspathic): 10 to 15 years on average, with documented cases beyond 20 years.
- Composite: 5 to 7 years, the shortest of the mainstream materials.
A full survival-rate breakdown by material covers how long do veneers last with 10-year and 20-year prospective data.
How Do Veneer Types Compare for Cost, Durability, and Aesthetics?
Veneer types diverge across three decision variables: feldspathic porcelain leads on aesthetics, lithium disilicate and zirconia lead on durability, and composite leads on price. The comparison table below pulls these variables together, with costs reflecting average ranges for international patients in Istanbul.
| Veneer type | Aesthetics | Durability | Repairability | Cost (per tooth, Istanbul range) |
|---|---|---|---|---|
| Porcelain (feldspathic) | Highest natural translucency | 10–15 years | Replace only | €€€ |
| Lithium disilicate (E.max) | High translucency, high strength | 12–20 years | Replace only | €€€–€€€€ |
| Composite (direct) | Acceptable, fades over time | 5–7 years | Chairside repair | € |
| Zirconia | Slightly opaque, very strong | 15+ years | Replace only | €€€€ |
| No-prep / Lumineers | Good, natural enamel retained | 10–20 years | Replace only | €€€ |
Aesthetic priority points toward feldspathic porcelain or lithium disilicate, budget priority points toward composite, and bruxism or a heavy bite points toward lithium disilicate or zirconia.
How Should Patients Choose Between Veneer Types?
The choice between veneer types is driven by four clinical variables: aesthetic priority, durability requirement, preparation tolerance, and budget. The framework below maps each priority to the material that fits it.
- Aesthetic priority is highest: Choose feldspathic porcelain or lithium disilicate for maximum translucency and shade depth.
- Durability priority is highest: Choose lithium disilicate or zirconia, especially for bruxers or full-arch cases.
- Tooth structure must be preserved: Choose no-prep porcelain or Lumineers, provided the case suits a minimal-bulk design.
- Budget is the main constraint: Choose composite veneers, accepting a shorter lifespan and periodic polishing.
- Erosion is on the back of the upper teeth: Choose palatal veneers to halt acid wear and restore lost structure.
- The restoration must be removable or short-term: Choose snap-on veneers for cosmetic events only, not as a clinical solution.
The right choice is rarely the strongest or cheapest material in isolation; it is the material that matches the patient’s bite, enamel coverage, aesthetic goal, and budget, confirmed with a diagnostic mock-up and Digital Smile Design preview before commitment.
How Does Digital Smile Design Influence the Choice of Veneer Type?
Digital Smile Design (DSD) influences the choice of veneer type by quantifying tooth proportions, smile line, and occlusal contacts before any material is selected. A digital preview shows whether the case needs the bulk of feldspathic porcelain, the strength of lithium disilicate, or the conservativeness of no-prep ceramic.
By letting the patient see the planned result on screen before preparation begins, Digital Smile Design reduces the risk of a mismatch between patient expectation and clinical outcome, since shape and shade are agreed on the digital plan rather than after the teeth are prepared.
Why Choose Vera Smile for Veneer Treatment?
Vera Smile is an international dental clinic in Istanbul that offers every clinically recognised veneer type under one digital workflow, with material selection matched to the patient’s bite, enamel status, and aesthetic priority rather than to a default brand or technique. The clinic operates under Republic of Turkey Ministry of Health authorisation and follows Slow Dentistry Global Network standards, which mandate isolation, time-controlled bonding, and disinfection protocols that protect veneer longevity. Cosmetic accuracy is supported by AACD-aligned expertise in shade and smile design, Digital Smile Design built into every full-arch case before material is selected, and 3D intraoral scanning with CAD/CAM dentistry for marginal accuracy in the 20–50 micron range.
Treatment planning at this dental clinic in Istanbul is designed to be transparent and evidence-based. Every patient receives a written plan with side-by-side images, lifespan projections, and cost ranges, allowing veneer options to be compared on objective criteria before any treatment begins. International patients also benefit from dedicated coordination covering airport transfers, accommodation, scheduling, and remote aftercare, helping ensure continuity of care after they return home.
FAQ
Yes, in selected cases. A single tooth may receive a different material to meet a specific clinical demand, for example a zirconia veneer on a heavily loaded canine alongside lithium disilicate on the incisors. Combining materials requires careful shade matching because each ceramic reflects light slightly differently.
Feldspathic porcelain veneers look the most natural, with lithium disilicate a very close second. The layered feldspathic ceramic reproduces the light scatter of enamel more faithfully than any other material, while lithium disilicate is preferred in most modern cases because it pairs a near-identical natural appearance with markedly higher strength.
Yes, in most cases. No-prep veneers bonded over intact enamel can be removed and the underlying tooth left structurally intact. Reversibility depends on whether any enamel was reshaped during placement and on the cement type used, and adhesive cement removal still requires careful instrumentation.
Composite veneers and no-prep porcelain veneers are the most comfortable for patients with pre-existing sensitivity, because both involve minimal or zero preparation. Composite limits sensitivity at placement through its minimal preparation depth, while no-prep porcelain removes no enamel at all, making it the most conservative option for sensitive teeth. A pre-treatment desensitising protocol may also be recommended before either option.
Yes, staining resistance varies sharply by material. Composite veneers stain faster than any ceramic because the resin matrix is more porous, whereas porcelain and lithium disilicate are nearly stain-proof on the bonded surface, though the cement margin can discolour over time, especially in smokers or heavy coffee drinkers.
Yes. When veneers are replaced, the patient and dentist can switch material based on updated clinical needs. A patient who originally chose composite may upgrade to lithium disilicate at the next cycle, or a patient with developing bruxism may move from feldspathic porcelain to zirconia for added strength.