
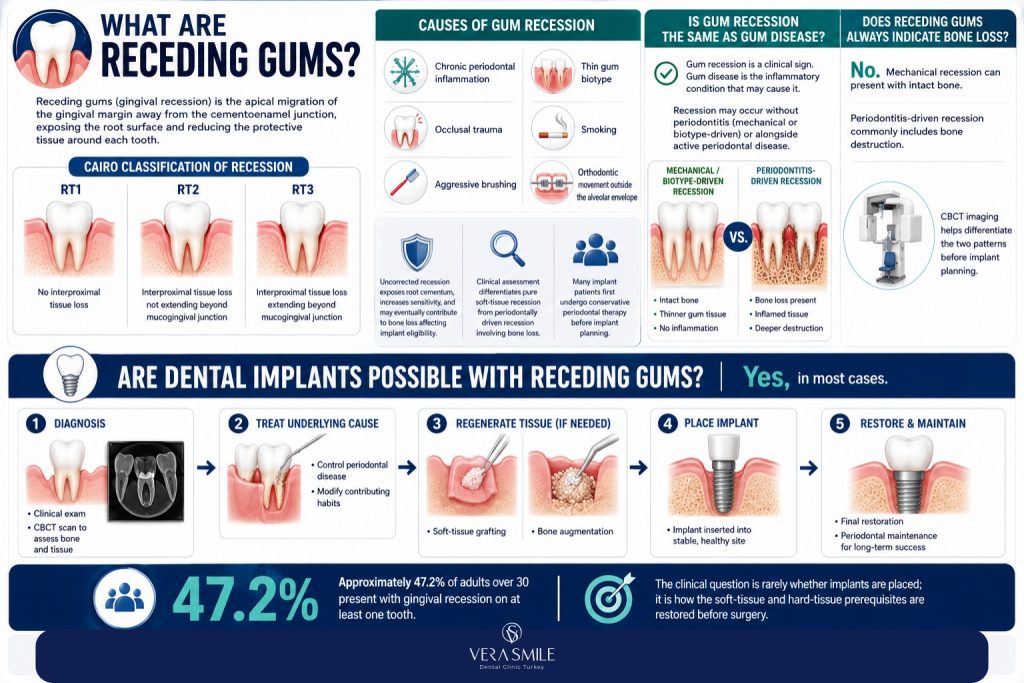
Yes, dental implants are possible for patients receding gums in most cases, provided the underlying bone volume is adequate, periodontal disease is controlled, and the soft-tissue defect is corrected before or during implant surgery. Receding gums alone do not disqualify a patient. The decisive factor is whether bone has been lost alongside the gum tissue. When bone loss is present, soft-tissue grafting and bone augmentation are performed first, then the implant is placed in a clinically stable site.
Approximately 47.2% of adults over 30 in the United States present with gingival recession on at least one tooth, according to the American Academy of Periodontology, and a growing share of these patients are simultaneously evaluated for dental implants. The clinical question is rarely whether implants are placed; it is how the soft-tissue and hard-tissue prerequisites are restored before surgery.
What Are Receding Gums?
Receding gums (gingival recession) is the apical migration of the gingival margin away from the cementoenamel junction, exposing the root surface and reducing the protective tissue around each tooth. Recession is graded using the Cairo classification (RT1, RT2, RT3) according to the degree of interproximal tissue loss visible on examination.
The condition develops from chronic periodontal inflammation, occlusal trauma, aggressive brushing, thin gum biotype, smoking, or orthodontic movement outside the alveolar envelope. Uncorrected recession exposes the root cementum, raises sensitivity, and over time produces underlying bone loss that affects the eligibility of the site for implant placement.
A full clinical assessment differentiates pure soft-tissue recession (intact bone) from periodontally driven recession (bone loss alongside tissue loss). The two scenarios carry different implant treatment pathways. Patients exploring the broader clinical context of gum recession arrive at implant planning after one or more cycles of conservative periodontal therapy.
Is Gum Recession the Same as Gum Disease?
No. Gum recession is a clinical sign; gum disease (gingivitis or periodontitis) is the inflammatory pathology that frequently produces it. Recession occurs in patients without periodontitis (mechanical or biotype-driven recession) and in patients with active periodontitis (inflammation-driven recession). The treatment pathway depends on the underlying cause.
Does Receding Gums Always Indicate Bone Loss?
No. Mechanical recession from aggressive brushing or thin biotype presents with intact underlying bone. Periodontitis-driven recession almost always involves bone loss because the inflammation destroys both soft and hard tissue. CBCT imaging is the only reliable way to differentiate the two patterns before implant planning.
Who Can Get Dental Implants With Receding Gums?
Yes, dental implants are placed in patients with receding gums when the supporting bone is adequate or restored, periodontal infection is controlled, and the soft-tissue envelope around the planned site is thickened to a stable architecture. Recession by itself is not a contraindication; the determining variables are bone volume, biotype, and infection status. Three patient categories define eligibility:
- Eligible Without Preparatory Soft-Tissue Surgery: Mild recession (RT1) with a thick gum biotype, intact bone, and no active periodontal inflammation allows implant placement under standard protocol.
- Eligible After Preparatory Grafting: Moderate recession (RT1–RT2) with thin biotype, partial bone loss, or shallow vestibule requires a connective tissue graft, free gingival graft, or guided bone regeneration to restore the site before implant placement.
- Conditional Eligibility (Specialist Evaluation Required): Severe recession (RT3) combined with advanced periodontitis, vertical bone loss, or systemic factors such as uncontrolled diabetes, immunosuppression, or heavy smoking requires staged periodontal stabilisation, regenerative surgery where indicated, and re-evaluation before implant planning.
A panoramic radiograph and a CBCT scan establish the bone profile of the planned site for dental implants. Probing depth, bleeding-on-probing scores, and biotype assessment establish the soft-tissue profile. Both data sets are required before treatment is finalised.
How Do Receding Gums Affect Implant Eligibility?
Receding gums affect dental implant eligibility through three connected variables: residual bone volume around the planned site, thickness of the keratinised gingival band, and the presence or absence of active periodontal infection. Each variable is measurable, and each carries a defined corrective protocol.
- Residual Bone Volume: A dental implant requires at least 1.5 mm of bone on the buccal aspect of the fixture and 6 mm of bone height to anchor a standard-diameter implant. Recession often progresses with horizontal or vertical bone loss; a CBCT scan quantifies what remains. Sites below this threshold need bone grafting before implant placement.
- Keratinised Gum Thickness: A keratinised band thinner than 2 mm around an implant correlates with higher rates of peri-implant recession and inflammation. Thin biotype patients receive a soft-tissue graft (subepithelial connective tissue graft or free gingival graft) to thicken the tissue before or during implant placement.
- Periodontal Infection Status: Active periodontitis is a contraindication to implant surgery. Probing depths above 4 mm, bleeding on probing above 20%, and radiographic bone loss require periodontal therapy through scaling, root planing, and reassessment until the disease is stable. A periodontal chart confirming pocket reduction below 4 mm is a prerequisite to implant scheduling.
- Smoking Status: Smokers carry a 2.6-fold increase in implant failure risk in recession-affected sites. Cessation for at least 4 weeks before and 8 weeks after surgery is the clinical standard.
Patients with periodontitis-driven recession benefit from structured periodontal treatment before any implant planning is finalised.
What Pre-Implant Treatments Restore a Recession-Affected Site?
Pre-implant treatments restore a recession-affected site through three categories of procedure: soft-tissue grafting to thicken the gum, bone grafting to rebuild lost volume, and periodontal therapy to control inflammation. The combination is selected after CBCT and clinical assessment.
| Pre-Implant Treatment | Indication | Healing Time | Cost in Turkey |
|---|---|---|---|
| Scaling and root planing | Active periodontitis | 4–6 weeks reassessment | €100 – €300 per arch |
| Connective tissue graft (CTG) | Thin biotype, root coverage | 6–8 weeks before implant | €250 – €600 per site |
| Free gingival graft (FGG) | Inadequate keratinised band | 8 weeks before implant | €200 – €500 per site |
| Guided bone regeneration (GBR) | Horizontal bone defect | 4–6 months before implant | €400 – €900 per site |
| Block bone graft (autogenous) | Vertical bone defect | 6 months before implant | €700 – €1,500 per site |
| Sinus lift (open or closed) | Posterior maxilla bone loss | 4–6 months before implant | €600 – €1,200 |
After regenerative procedures, the site is reassessed clinically and radiographically before implant placement is scheduled. Most patients combining gum and bone work need a 4–6 month preparatory window before fixture installation.
Are Soft-Tissue Grafting and Implant Placement Done at the Same Appointment?
Yes, in selected cases. Connective tissue grafting is performed at the same surgical visit as implant placement when the bone defect is small and primary stability of the implant is achievable. This single-stage protocol shortens treatment by 2–3 months. Larger bone defects require staged surgery: graft first, implant later, after complete healing.
How Does the Implant Procedure Differ for Patients With Receding Gums?
The implant procedure for patients with receding gums adds soft-tissue management at three stages: site preparation, fixture placement, and prosthetic emergence profile design. Standard implant protocol is preserved; the additions protect the long-term tissue contour around the restoration.
- Site preparation: A periodontal phase precedes surgical planning. Active disease is resolved before any incision is made. CBCT imaging defines the implant axis and depth that will sit within the rebuilt bone envelope.
- Soft-tissue augmentation at fixture placement: A subepithelial connective tissue graft is harvested from the palate and placed buccal to the implant during the same surgical visit when biotype is thin. This thickens the tissue and reduces the risk of marginal recession around the future restoration.
- Implant positioning: The fixture is placed slightly more palatally than in a non-recession case, providing buccal bone width and soft-tissue room for the prosthetic emergence profile.
- Healing protocol: A submerged (two-stage) healing approach is preferred for recession-affected sites. The implant heals under the gum for 3–6 months, isolated from oral bacteria, before the abutment is exposed.
- Prosthetic emergence profile: The crown is shaped with a flat or slightly concave emergence profile to support the gum architecture rather than displace it. Screw-retained crowns are preferred over cement-retained options to prevent residual cement triggering peri-implant inflammation.
For patients facing insufficient bone in the upper jaw despite grafting, zygomatic implants anchored in the cheekbone provide a documented alternative that bypasses deficient maxillary bone and avoids large-volume sinus augmentation.
Do You Need A Gum Graft Before Every Implant in A Patient With Recession?
No, a gum graft is required when the keratinised tissue at the planned site is thinner than 2 mm or when the biotype is thin enough to predict marginal recession around the future restoration. Thick-biotype patients with localised recession on a different tooth often receive the implant under standard protocol without grafting.
What Are the Risks of Dental Implants in Recession-Affected Sites?
Implants placed in recession-affected sites carry an elevated risk of peri-implant mucositis, peri-implantitis, marginal recession around the implant, and aesthetic compromise from exposed metal abutments. Risk control depends on tissue augmentation, periodontal maintenance, and prosthetic design.
- Peri-implant mucositis: Inflammation of the soft tissue around the implant without bone loss. Reported in 43% of implants at 5-year follow-up; reversible with hygiene control and professional cleaning.
- Peri-implantitis: Inflammation with progressive bone loss around the implant. Reported in 22% of patients at 5-year follow-up; the leading cause of late implant failure. Prior periodontitis triples the baseline risk.
- Marginal recession around the implant: The gum tissue migrates apically, exposing the abutment-implant junction. Aesthetic and functional concern in the front zone of the mouth.
- Black triangles: Loss of papilla between the implant and adjacent teeth, producing visible spaces beneath the contact point. Common when interproximal bone is reduced.
- Implant failure: The fixture loses osseointegration and is removed. Failure rates rise from 1–2% in healthy patients to 4–7% in patients with prior periodontitis.
For broader context on long-term implant outcomes, the documented patterns of dental implant complications cover the full risk spectrum.
Do Receding Gums Cause Implants to Fail?
Receding gums alone do not cause implant failure. The underlying drivers (active periodontitis, smoking, inadequate bone, thin biotype) are what raise failure risk. When these drivers are controlled before surgery, implants in patients with prior recession achieve survival rates of 90–95% at 10 years, in line with standard implant cases.
How Much Do Dental Implants With Receding Gums Cost in Turkey?
Dental implants combined with gum and bone treatment in Turkey cost between €450 and €2,800 per implant site, depending on the complexity of the soft-tissue and hard-tissue work required. A straightforward implant in a recession-eligible site sits at the lower end; staged grafting plus implant placement approaches the upper end.
| Treatment Stage | Cost in Turkey | UK Equivalent | US Equivalent |
|---|---|---|---|
| Standard single dental implant | €350 – €900 | £1,800 – £3,000 | $3,500 – $5,500 |
| Connective tissue graft (per site) | €250 – €600 | £600 – £1,200 | $800 – $2,000 |
| Free gingival graft (per site) | €200 – €500 | £500 – £1,000 | $700 – $1,800 |
| Guided bone regeneration | €400 – €900 | £800 – £1,500 | $1,200 – $3,000 |
| Sinus lift | €600 – €1,200 | £1,200 – £2,500 | $1,500 – $5,000 |
| Periodontal therapy (full mouth) | €200 – €500 | £600 – £1,200 | $1,000 – $3,500 |
| Combined site (implant + soft-tissue graft) | €600 – €1,500 | £2,400 – £4,200 | $4,300 – $7,500 |
| Combined site (implant + GBR + soft-tissue graft) | €1,000 – €2,800 | £3,200 – £5,500 | $5,500 – $10,000 |
A more granular per-implant breakdown is published in the dedicated guide on dental implant cost in Turkey. The Turkey price reflects lower laboratory and operational overhead rather than reduced clinical standards. Internationally accredited Turkish clinics use the same implant systems (Straumann, Nobel Biocare), the same regenerative materials, and the same surgical protocols as their UK and US counterparts.
Is the Turkey Package All-Inclusive for Combined Gum and Implant Treatment?
Reputable internationally accredited clinics in Istanbul present a single package price covering CBCT imaging, surgical planning, all surgical procedures, regenerative materials, temporary restorations, abutments, final crowns, and post-treatment review. Hotel accommodation and VIP airport transfer are included for international patients. The patient’s flight is the only excluded item in most published packages.
How Long Does Combined Treatment for Implants and Receding Gums Take?
Combined treatment for receding gums and dental implants takes between 3 and 9 months from initial consultation to final crown delivery, depending on whether grafting is performed in stages or simultaneously with implant placement. International patients structure the timeline across two or three trips to Istanbul.
- Periodontal stabilisation phase (4–6 weeks): Scaling, root planing, oral hygiene reinforcement, and reassessment. Performed remotely with a local periodontist or in a first short visit to Istanbul.
- Soft-tissue grafting phase (6–8 weeks healing): Connective tissue graft or free gingival graft followed by tissue maturation. The first Istanbul trip covers 7–10 days.
- Bone grafting phase (4–6 months healing, when needed): Guided bone regeneration or block grafts followed by complete bone integration. Performed at the same visit as soft-tissue grafting where the case allows.
- Implant placement phase (3–6 months osseointegration): Surgical fixture placement under local anaesthesia, followed by submerged healing. The second Istanbul trip covers 3–5 days.
- Prosthetic phase (2–3 weeks): Abutment connection, impression or scan, and final crown delivery. The third Istanbul trip covers 5–7 days.
Single-stage protocols (graft and implant in the same surgical visit) compress the total timeline to 4–5 months for selected cases.
How Many Trips Does Combined Treatment Require?
The number of Istanbul trips depends on whether soft-tissue and bone procedures are staged or simultaneous. Most combined cases require two to three visits across the full treatment period.
| Treatment Pathway | Total Treatment Time | Number of Istanbul Trips |
|---|---|---|
| Implant only (mild recession, intact bone) | 3–4 months | 2 trips |
| Implant + simultaneous soft-tissue graft | 4–5 months | 2 trips |
| Implant + staged soft-tissue graft | 5–6 months | 2–3 trips |
| Implant + GBR + soft-tissue graft | 7–9 months | 3 trips |
Single-stage protocols compress total duration by eliminating the separate soft-tissue healing window, but require confirmed primary implant stability at placement.
How Are Receding Gums Around Existing Implants Treated?
Recession around an existing implant is treated through soft-tissue grafting, decontamination of the exposed implant surface, prosthetic redesign, or implant replacement, depending on the cause and severity. Early identification protects the long-term outcome.
- Connective tissue grafting: A subepithelial CT graft is placed at the buccal aspect of the recessed implant to thicken the tissue and partially cover the exposed margin. Aesthetic improvement is partial; complete root coverage of the implant is harder to achieve than around natural teeth.
- Implant surface decontamination: When peri-implantitis is the driver, mechanical and chemical decontamination of the exposed threads (titanium brushes, glycine air-polishing, chlorhexidine, citric acid) is performed before any soft-tissue procedure.
- Prosthetic correction: A new crown with a modified emergence profile reduces tissue compression and supports the soft-tissue contour without forcing displacement.
- Implant explantation and replacement: When peri-implantitis has progressed beyond reversal or the implant is malpositioned, removal of the fixture and staged regeneration allows a new implant to be placed in a corrected site.
The relevant warning signs are documented in the broader pattern of dental implant failure, and routine monitoring at six-month intervals identifies the early changes before bone loss progresses.
Who Is the Right Candidate for Implants When Gums Are Receding?
The ideal candidate has localised recession in a healthy periodontal environment, sufficient bone volume confirmed on CBCT, a thick or augmentable biotype, controlled systemic health, and willingness to maintain a strict hygiene protocol post-surgery. Clinical assessment confirms suitability before any treatment is committed.
- Localised Mechanical Recession: Patients with intact alveolar bone confirmed on CBCT and no active periodontitis are eligible for implant placement under standard protocol.
- Treated Periodontitis: Former periodontitis patients with stable probing depths under 4 mm and completed maintenance therapy qualify for implant planning.
- Non-Smoker or Pre-surgical Cessation: Non-smokers or patients willing to stop at least 4 weeks before and 8 weeks after surgery show significantly lower failure rates at recession-affected sites.
Weak candidate profile includes patients with active untreated periodontitis, heavy smokers unwilling to stop, patients with severe vertical bone loss across multiple sites, patients with uncontrolled diabetes or immunosuppression, and patients with a history of repeated implant failure due to peri-implantitis. For older patients, the age-specific eligibility framework is covered under dental implants for seniors.
Why Do International Patients Choose Vera Smile for Implants With Receding Gums?
Patients with receding gums require more than standard implant placement. Successful outcomes depend on precise periodontal management, bone support, and long-term tissue stability. International patients evaluating treatment options focus on clinics that combine surgical accuracy with structured care pathways.
- International Accreditation: Vera Smile operates as an internationally accredited dental clinic in Istanbul, delivering implant surgery and periodontal regeneration through integrated multidisciplinary planning. Clinical protocols align with European and US periodontal and implant guidelines, ensuring consistent surgical standards for patients with receding gums.
- Specialist-Led Approach: Treatment is performed by a coordinated team that includes a periodontist, oral surgeon, prosthodontist, and master ceramist. Each specialist contributes to a single, unified treatment plan, eliminating fragmentation in complex implant and gum reconstruction cases.
- CBCT-Driven Planning: All procedures are based on a CBCT-supported diagnostic workflow, allowing precise assessment of bone volume, gum recession severity, and implant positioning. This approach reduces surgical uncertainty and improves long-term stability.
- Integrated Treatment Timeline: Combined periodontal and implant cases are completed within 4–9 months across two or three structured visits, compared to 9–14 months in systems where treatments are divided across multiple clinics.
- Advanced Case Capability: Patients requiring more complex solutions, including full-arch rehabilitation, All-on-4 dental implants, or zygomatic implants, receive treatment within a single coordinated clinical pathway, even in cases involving severe maxillary atrophy.
- All-Inclusive International Care: The treatment pathway includes hotel accommodation, VIP airport transfers, and multilingual coordination. Post-treatment care is structured with remote follow-ups at 1 week, 1 month, and 6 months, supported by a detailed written aftercare protocol in English.
- Cost Efficiency With Clinical Consistency: For patients comparing global options, treatment through dental tourism in Turkey delivers a 50–70% cost reduction relative to UK and US pricing, without deviation from established international implant and periodontal standards.
Vera Smile positions implant treatment within a fully integrated system, where diagnosis, surgery, and restoration follow a single coordinated plan.