
Tooth sensitivity (15–78% of patients) and gum irritation (around 25%) are the most common side effects of teeth whitening, and both are temporary when products are used as directed. Less common but more serious risks, including enamel demineralisation, pulp inflammation, and cervical root resorption, are tied to high concentrations, overuse, or use on contraindicated teeth rather than to routine whitening. Whitening also creates a colour mismatch with existing veneers, crowns, and composite fillings, none of which lighten. Long-term data on standard 10% carbamide peroxide shows no clinically significant pulp or enamel damage with normal use. Risk rises with concentration and exposure time, which is why in-office and LED or UV systems carry a sharper sensitivity profile than low-strength strips. Certain groups, including children, pregnant women, and people with untreated decay or gum disease, should not whiten until a dentist has assessed them. Most side effects are preventable with a structured pre-treatment protocol.
What Are the Side Effects of Teeth Whitening?
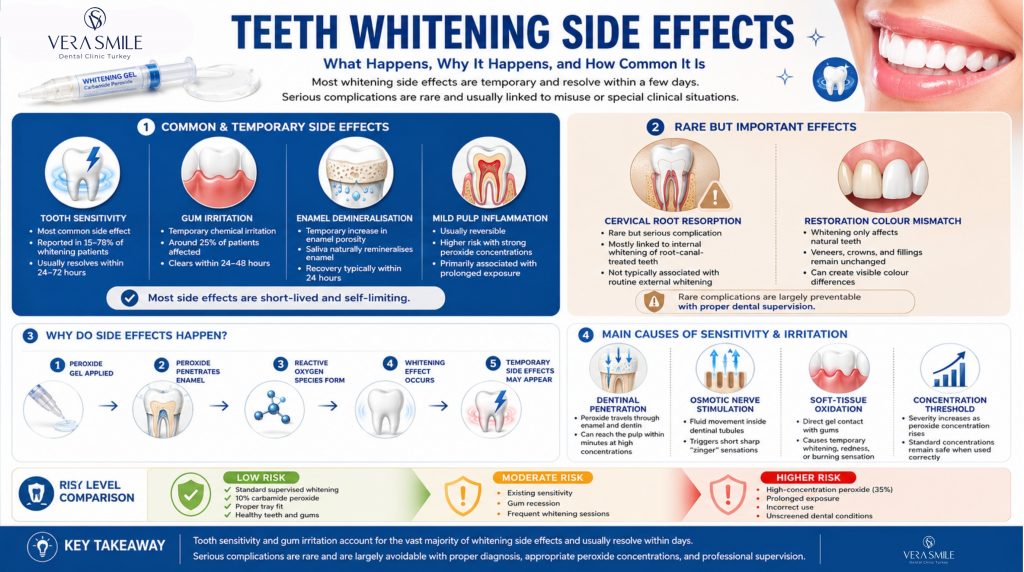
Teeth whitening side effects fall into two groups: common and temporary, or rare and potentially lasting. Tooth sensitivity and gum irritation account for almost all reported cases and resolve within days, while the remaining effects are uncommon and linked to specific misuse patterns or pre-existing conditions.
- Tooth sensitivity: The most common effect, reported in 15–78% of external bleaching patients and resolving within 24–72 hours of stopping treatment (British Dental Journal, 2006).
- Gum irritation: Temporary chemical irritation of the soft tissue affecting around 25% of patients and clearing within 24–48 hours.
- Enamel demineralisation: A shallow, temporary increase in enamel porosity that saliva remineralises within about 24 hours at standard concentrations.
- Pulp inflammation: A mild, reversible response at clinical concentrations that becomes a genuine risk only with 35% hydrogen peroxide and prolonged exposure.
- Cervical root resorption: A rare but serious complication associated almost exclusively with internal bleaching of root-canal-treated teeth.
- Restoration colour mismatch: A permanent shade difference that appears when natural teeth lighten but adjacent veneers, crowns, or composite fillings do not.
The common effects are short-lived and manageable; the serious ones are largely avoidable by using standard concentrations and screening for contraindications first.
What Are the Causes of Teeth Whitening Side Effects?
Teeth whitening side effects are caused by peroxide penetrating enamel and dentin, where it disturbs nerve fibres, oxidises soft tissue, and at high concentrations reaches the pulp. Both hydrogen peroxide (H2O2) and carbamide peroxide (CP) break down into reactive oxygen species that drive whitening and, as a by-product, the side effects, with concentration the single variable that determines severity.
- Dentinal penetration: Peroxide passes through enamel and travels along open dentinal tubules toward the pulp, reaching it within 15 minutes at 35% H2O2.
- Osmotic nerve stimulation: The concentration gradient shifts the fluid inside the tubules, which stimulates A-delta nerve fibres and produces the brief, sharp pain known as zingers.
- Soft-tissue oxidation: Direct gel contact oxidises unkeratinised gum tissue, causing temporary whitening, redness, or a burning sensation.
- Concentration threshold: 10% carbamide peroxide equals roughly 3.3% hydrogen peroxide, a level safe for enamel and pulp when used as directed (Journal of the American Dental Association, 2002).
Because the mechanism is dose-dependent, the same agent produces minimal effects at low concentrations and meaningful risk at high ones.
Why Does Tooth Sensitivity Happen After Teeth Whitening?
Tooth sensitivity happens because peroxide moves the fluid inside the dentinal tubules, which stimulates the A-delta nerve fibres in the pulp. It is the dominant complaint across all whitening methods, appearing within hours of the first session and peaking during treatment, and it ranges from mild cold sensitivity to sharp, spontaneous zingers that last one to two seconds. Research in the British Dental Journal (2006) recorded sensitivity in 15% to 78% of external bleaching patients, with the wide range reflecting individual anatomy: larger tubule diameter, thinner enamel, and existing gum recession all raise the risk.
How Long Does Whitening Sensitivity Last?
Whitening sensitivity lasts 24 to 72 hours after most at-home treatments and up to seven days after high-concentration in-office sessions. Duration depends mainly on the method and peroxide concentration used, as shown below.
| Method | Sensitivity Duration | Peak Severity |
|---|---|---|
| Whitening strips (10% CP) | 24–48 hours post-session | Mild to moderate |
| At-home trays (10–22% CP) | 24–72 hours | Mild to moderate |
| In-office (25–40% H2O2) | Up to 7 days | Moderate to severe |
| Zoom / lamp-assisted | 24–48 hours with pre-treatment | Moderate |
| Whitening pen (low concentration) | Minimal to none | Mild |
Sensitivity that persists beyond two weeks is not normal and warrants a dental evaluation, since it can signal exposed dentin, an untreated cavity, or early irreversible pulpitis.
Why Do Some People Experience More Sensitivity Than Others?
Sensitivity varies between people because enamel thickness, dentinal tubule density, and salivary buffering capacity differ from person to person. People with thick, well-mineralised enamel and tighter tubule junctions often feel little or no sensitivity, even at higher concentrations, while those with thin enamel, wider tubules, or gum recession feel more. This is why two people using the same strips on the same night can have completely different experiences. A strong natural salivary buffer also neutralises the peroxide gradient faster and shortens the sensitive window.
Can Teeth Whitening Irritate the Gums?
Yes, teeth whitening can irritate the gums when peroxide gel contacts soft tissue, producing temporary whitening, redness, or a burning sensation. Gum irritation is the second most common whitening side effect. Hydrogen peroxide is an oxidising agent, and the soft, unkeratinised tissue between the teeth reacts to direct contact with a superficial chemical irritation. The cause is almost always the same: gel reaches the gum through an ill-fitting tray, an overfilled strip, or too much gel. In a dental setting the gums are protected with a rubber dam or liquid dam before any agent is applied; at home, no such barrier exists.
When Does Gum Irritation Become Serious?
Gum irritation becomes serious only when gel contact is repeated or prolonged, such as a tray worn overnight for several consecutive nights or a heavily overfilled strip left on for twice the recommended time. Mild irritation (white patches, tenderness, slight swelling) resolves within 24 to 48 hours without treatment. If gum whitening or sores persist beyond 72 hours, or if ulceration, jaw-radiating pain, or non-stop bleeding develops, stop whitening and see a dentist, because these are not normal whitening effects.
What Are the Long-Term Side Effects of Teeth Whitening?
The long-term side effects of teeth whitening are minimal at standard concentrations, but high-concentration overuse can cause permanent enamel loss, irreversible pulp damage, or cervical root resorption. A seven-year clinical follow-up found that no patient treated with a standard 10% carbamide peroxide system required root canal treatment on whitened teeth, indicating no clinically significant pulp damage (Haywood et al., cited in JADA, 2002). The risk profile changes at higher concentrations and with repeated overuse.
- Enamel demineralisation: Standard products (10–22% CP) cause shallow, temporary demineralisation that saliva reverses within 24 hours, while permanent loss requires repeated 35%+ H2O2 use, application to already-thin or eroded enamel, or daily abrasive whitening pastes alongside bleaching (ADA, 2010).
- Irreversible pulp damage: At 10–22% CP the pulp response is mild and reversible, but 35% H2O2 with heat or light and prolonged application can trigger irreversible pulpitis, since a 2021 study in Scientific Reports linked high concentration and 4+ hour exposure to reduced pulp cell viability.
- Cervical root resorption: This progressive destruction of the root from the outside is rare and almost exclusive to internal bleaching of non-vital teeth, where high-concentration H2O2 and heat reach the external root surface (British Dental Journal, 2006).
- Enamel non-regeneration: Any enamel genuinely lost does not return, because ameloblasts, the enamel-forming cells, are shed after the tooth erupts.
At consumer and dentist-supervised concentrations the long-term outlook is reassuring; the permanent outcomes are confined to misuse, very high strengths, and internal bleaching.
Do LED and UV Teeth Whitening Systems Cause More Side Effects?
Yes, some LED and UV systems can increase intra-session sensitivity, though the light itself is not the underlying cause: certain lamps generate heat at the pulp, while the overall safety profile is set by the peroxide concentration. These systems (including Zoom, at-home LED kits, and lamp-activated professional units) add a light source meant to speed up activation of the peroxide. A 2021 study in BMC Oral Health found the efficacy benefit of light unclear, while the thermal effect is well documented: certain wavelengths raise dentin temperature, increase tubule fluid movement, and intensify zingers during treatment. Post-treatment sensitivity runs higher with lamp-activated systems than with gel-only methods, particularly at 30–40 minute exposure windows. UV wavelengths also pose an eye risk, so reputable in-office systems require eye protection, and most at-home kits use lower-risk blue-spectrum light rather than UV.
What Are the Zoom Teeth Whitening Side Effects?
Zoom whitening’s main side effects are sharp intra-session zingers and 24–48 hours of post-session sensitivity, because it uses a 25% hydrogen peroxide gel activated by a lamp over three 15-minute cycles. It is one of the fastest in-office systems (about 45 minutes of chair time) and carries a more pronounced sensitivity profile than tray-based whitening. Its characteristic effects are below.
- Intra-session zingers: Sharp A-delta nerve responses to rapid fluid shifts, reported by roughly 10–20% of patients during lamp activation and lasting under two seconds.
- Post-session sensitivity: Lasts 24–48 hours in most patients and responds to desensitising toothpaste or potassium nitrate gel applied immediately afterward.
- Gum blanching: Localised gum whitening where liquid dam protection is imperfect, resolving within hours.
- Reversible pulpitis: A rare thermal and chemical response to 25% H2O2 under lamp activation, marked by spontaneous pain lasting minutes rather than seconds, which is temporary and does not indicate nerve death.
Two weeks of desensitising toothpaste before treatment and a 10-minute application of 5% potassium nitrate gel beforehand measurably lower the chance of sensitivity.
What Are the Side Effects of Whitening Strips?
Whitening strips mostly cause mild tooth sensitivity and gum soreness, because most use a low 6–10% hydrogen peroxide gel. Strips are the most widely used at-home product, and their lower concentration keeps the side-effect profile mild. The most common effects are listed below.
- First-day sensitivity: Mild tooth sensitivity that is most noticeable during the first two days of use.
- Gum soreness: Whitening or soreness where the strip overlaps gum tissue, avoidable by placing strips 1–2 mm from the gumline.
- Uneven whitening: Patchy results on crooked or overlapping teeth, where the gel cannot reach inner surfaces.
- Restoration mismatch: Lightening of natural teeth while composite fillings shift only slightly and porcelain stays unchanged, producing a colour difference.
- Increased microleakage: A temporary rise in leakage at the tooth-filling margin, relevant for people with large composite restorations.
Strips should not be used over composite bonding, ceramic veneers, or dental crowns, because peroxide cannot penetrate ceramic or metal and the resulting shade mismatch is not reversible without replacing the restoration.
Who Should Not Whiten Their Teeth?
Whitening is not appropriate for children under 16, pregnant or breastfeeding women, or anyone with untreated decay, active gum disease, exposed roots, a peroxide allergy, or tetracycline staining. These groups face elevated risk and should consult a dentist before using any bleaching product, for the reasons set out below.
- Children under 16: The proportionally larger pulp chamber sits closer to the enamel, so peroxide reaches living tissue faster and the ADA advises against whitening this group (ADA, 2010).
- Pregnant and breastfeeding women: With no long-term human safety data on peroxide during pregnancy, the precautionary advice is to defer whitening until after weaning.
- Active gum disease: Receded, inflamed gums expose root dentin that lacks an enamel barrier, which sharply increases sensitivity and tissue reaction, so periodontitis must be treated first.
- Exposed root surfaces: Cementum is thinner and more permeable than enamel, so gel reaches root dentin and the pulp quickly while achieving little whitening.
- Untreated cavities: Peroxide enters carious lesions directly and reaches the pulp unimpeded, causing acute pain, so all cavities should be filled before whitening.
- Peroxide allergy: A rare but real reaction ranging from hives and oral swelling to anaphylaxis in severe cases.
- Tetracycline-stained teeth: This intrinsic dentin staining responds poorly to bleaching and may need months of nightly trays or, in severe cases, veneers or crowns.
Where a contraindication applies, the underlying condition is treated first and a dentist confirms suitability before any whitening begins.
Does Whitening Affect Dental Restorations, Veneers, or Crowns?
No, whitening does not change the colour of restorations: porcelain veneers, ceramic and zirconia crowns, metal amalgam, and gold are unaffected, because the agents act only on the colour-causing molecules inside natural enamel and dentin.
The practical problem arises with tooth-coloured composite resin: peroxide makes composite absorb moisture and shift temporarily lighter, reduces the surface hardness of the material, and increases microleakage at the restoration margin (MDPI Applied Sciences, 2023). For anyone with composite bonding on visible front teeth, the sequence matters: whiten first, then replace the bonding at the new shade, or weigh whether porcelain veneers or dental crowns at the target shade are a better long-term option. If a crown or veneer on a front tooth no longer matches after whitening, the mismatch can only be corrected by replacing the restoration.
Does Teeth Whitening Affect the Oral Microbiome?
Yes, teeth whitening can shift the oral microbiome because hydrogen peroxide is antimicrobial, but at standard frequencies (one to two professional sessions a year) the clinical impact on healthy patients is low. Repeated peroxide exposure reduces some beneficial bacteria and favours peroxide-resistant strains, and the relevance depends on the patient’s baseline oral health.
| Patient profile | Microbiome impact | Recommendation |
|---|---|---|
| Healthy mouth, 1–2 sessions per year | Minimal, self-correcting | No special precaution needed |
| Frequent OTC plus daily whitening toothpaste | Cumulative shift in bacterial balance | Reduce frequency and consult a dentist |
| Active caries or periodontitis | Higher risk of worsening imbalance | Treat the condition before whitening |
| Dry mouth (low saliva) | Slower recovery of normal flora | Manage dryness and space sessions |
For most people the microbiome effect is not a practical concern; it matters mainly for those combining frequent products or whitening over an unmanaged oral condition.
Are Teeth Whitening Side Effects Permanent?
Most teeth whitening side effects are temporary and resolve within days, while a small number are permanent and tied to overuse or internal bleaching. The distinction depends on the mechanism: reversible fluid and inflammatory responses fade, but lost enamel and resorbed root structure do not, as the table shows.
| Side effect | Temporary or permanent |
|---|---|
| Tooth sensitivity | Temporary (24–72 h) with correct use |
| Gum irritation or whitening | Temporary (24–48 h) |
| Enamel demineralisation | Temporary, remineralises within 24 h via saliva |
| Composite resin softening | Temporary, surface hardness recovers in 7–14 days |
| Reversible pulpitis | Temporary, resolves in days to weeks |
| Enamel loss from overuse | Permanent, enamel does not regenerate |
| Irreversible pulpitis or nerve death | Permanent, requires root canal |
| Cervical root resorption (internal bleaching) | Progressive and permanent if untreated |
| Restoration colour mismatch | Permanent until the restoration is replaced |
The permanent outcomes share a common cause: high concentrations, repeated overuse, or treatment applied to teeth that should have been excluded, all of which are avoidable with correct use and screening.
How Can You Reduce Teeth Whitening Side Effects?
Most teeth whitening side effects are preventable by lowering exposure, blocking the dentinal tubules before treatment, and remineralising the enamel afterward. Each step below has clinical evidence behind it and can be combined for the best result.
- Pre-treat with potassium nitrate toothpaste: Using a KNO3 toothpaste for two weeks before whitening raises the threshold at which A-delta nerves fire and demonstrably reduces intra-session sensitivity.
- Apply 5% potassium nitrate gel before treatment: A 10-minute tray application fills the tubules with depolarised ions and buffers the osmotic shock when peroxide enters.
- Do not overfill the tray: Use the minimum gel that covers the tooth surface (around 0.25 ml per arch) and wipe any excess from the gums immediately.
- Use the shortest effective exposure: Start at the lower end of the product’s time range, since efficacy does not rise linearly with longer contact.
- Space out sessions: Leaving a day between sessions lets saliva remineralise the enamel and lowers cumulative oxidative load on the pulp.
- Remineralise with nano-hydroxyapatite toothpaste: n-HAp occludes the dentinal tubules and integrates into enamel, easing post-session sensitivity faster than fluoride alone (Journal of Dentistry, 2019).
- Take 400 mg ibuprofen before an in-office session: Taken 30 minutes beforehand, it reduces the prostaglandin-driven inflammatory component of post-session sensitivity.
Combining a pre-treatment desensitising protocol with post-session remineralisation addresses both the nerve and enamel pathways, which is how supervised whitening keeps side effects low.
Why Choose Professional Whitening in Turkey at Vera Smile?
At Vera Smile, every whitening treatment in Turkey begins with a full clinical assessment of gum health, enamel thickness, existing restorations, and sensitivity history. Where indicated, we apply a two-week desensitising protocol before any bleaching agent is used, protect the gums with a liquid dam during treatment, and finish with a nano-hydroxyapatite remineralisation step before you leave. This pre-treatment tubule-blocking and post-session remineralisation approach is built specifically to keep sensitivity low while delivering a stable, even result.
Vera Smile holds certification from the Republic of Turkey Ministry of Health and is a member of the American Academy of Cosmetic Dentistry, reflecting clinical standards and safety protocols that go beyond standard in-office care. For patients traveling for treatment, the same assessment, supervision, and aftercare apply throughout the whitening journey in Turkey.
FAQ
Yes, with modifications. Use a low concentration (6–10% H2O2 or 10% CP), shorten each session, pre-treat with potassium nitrate toothpaste for two weeks, apply n-HAp toothpaste after each session, and space sessions further apart, because sensitivity is dose- and time-dependent.
No. Standard strips (6–10% H2O2) cause temporary surface demineralisation that saliva reverses within 24 hours, and long-term studies of 10% carbamide peroxide show no measurable change in enamel hardness with normal use. Permanent damage requires sustained overuse at high concentrations.
No, not with standard products. A seven-year study found zero root canal treatments among patients whitened with 10% carbamide peroxide, indicating no clinically significant pulp damage. High-concentration treatments without proper time limits carry a small but real risk of irreversible pulpitis that could in theory progress to needing a root canal.
Because hydrogen peroxide temporarily blanches soft tissue on contact, the same way an antiseptic does on skin. The white colour is a superficial oxidation reaction, not damage, and it clears within 30–60 minutes. If it keeps happening, the strip is overlapping the gum, so place it 1–2 mm from the gumline.
No. The lamp does not make whitening safer; it is added to speed up activation, and safety depends on the peroxide concentration. Some heat-generating lamps can increase sensitivity compared with gel alone, and blue-spectrum LED is lower-risk than UV.
Because of temporary dehydration. Right after whitening the enamel is dehydrated and looks opaque and bright; as saliva rehydrates the tooth over 24–48 hours, natural translucency returns and the shade settles slightly darker. The settled shade is the real result, not the peak brightness seen in the chair.
It depends on the concentration. Small amounts of consumer gel (3–10% hydrogen peroxide) are low-risk and break down in saliva and stomach acid into water and oxygen, producing a foamy sensation but no systemic harm. Dentist-dispensed tray gel (10–22% carbamide peroxide) is stronger, so anyone who swallows a meaningful amount should drink water and watch for nausea. Professional-strength gel (35% hydrogen peroxide) is a medical emergency if a significant volume is ingested, causing nausea, vomiting, mucosal burns, and rarely oxygen embolism. In Turkey, if professional-strength gel is swallowed, contact the National Poison Information Centre (UZEM) on 114, or emergency services on 112.