
Dental implants are widely regarded as one of the most reliable solutions for replacing missing teeth, yet many patients still question whether people regret getting them. In practice, true regret is uncommon when diagnosis, surgical planning, and aftercare are handled properly. Most patients report stronger chewing function, clearer speech, and greater confidence compared to removable dentures or traditional bridges.
When dissatisfaction occurs, it is rarely about the implant concept itself. It is more connected to inadequate treatment planning, poor communication about healing timelines, unexpected financial pressure, surgical complications, or unrealistic expectations about immediate results. Dental implants require a surgical procedure, a defined healing period, and strict oral hygiene maintenance. Outcomes depend heavily on bone quality, systemic health, and clinical expertise.
Understanding whether regret develops requires evaluating clinical risk factors, recovery time, total treatment cost, and long-term maintenance responsibilities, rather than assuming implants inherently lead to dissatisfaction.
What Does “Regret” Actually Mean in Implant Dentistry?
In implant dentistry, regret is not a single, uniform experience. It reflects different forms of dissatisfaction that arise after treatment. Most discussions treat regret as a general feeling, yet it falls into three distinct categories: emotional regret, functional regret, and biological regret. Understanding this distinction clarifies why some patients feel uneasy despite technically successful treatment.
Emotional regret relates to decision anxiety or buyer’s remorse. A patient questions whether the financial investment was justified or feels stress about undergoing surgery. This form of regret is psychological rather than clinical. The implant itself remains stable, but the individual struggles with the weight of the decision, cost perception, or fear during recovery.
Functional regret involves dissatisfaction with chewing comfort, bite balance, or the way the prosthetic crown integrates with surrounding teeth. If occlusion is not adjusted precisely, patients experience pressure sensitivity, jaw fatigue, or difficulty adapting to the new tooth. Here, the issue centers on performance rather than emotion or infection.
Biological regret reflects genuine clinical complications such as inflammation around the implant, peri-implant bone loss, or mechanical failure of components. This category includes conditions like peri-implantitis, soft tissue recession, or loosening of abutments. Biological regret represents objective medical problems rather than perception alone.
Separating regret into these three categories provides clarity that is absent in most implant discussions. Not every feeling of dissatisfaction signals implant failure, and not every complication stems from poor surgical technique. Each category requires a different form of evaluation and response.
Why Do Some Patients Regret Dental Implants?
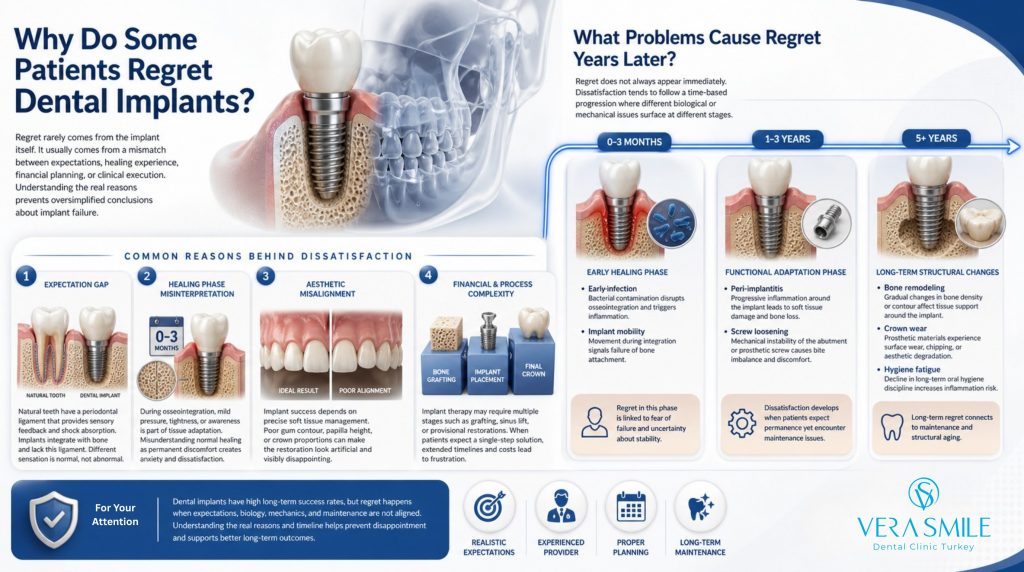
Although dental implants demonstrate high long-term success rates, a small percentage of patients report dissatisfaction after treatment. Regret rarely stems from the implant material itself. In most cases, it develops from a mismatch between expectations, healing experience, financial planning, or clinical execution. Understanding the structured reasons behind dissatisfaction provides clarity and prevents oversimplified conclusions about implant failure.
- Expectation Gap: Dental implants restore function and stability, yet they do not replicate the exact biological structure of a natural tooth. A natural tooth contains a periodontal ligament, which provides subtle sensory feedback and shock absorption. An implant integrates directly with bone and lacks this ligament. Some patients interpret this difference in sensation as abnormal, even though it reflects normal implant biomechanics.
- Healing Phase Misinterpretation: During osseointegration, mild pressure sensation, tightness, or awareness of the implant site is part of tissue adaptation. If this transitional phase is misunderstood as permanent discomfort, patients assume structural failure. Misreading normal healing responses creates unnecessary anxiety and dissatisfaction.
- Aesthetic Misalignment: Implant success depends not only on bone integration but on precise soft tissue management. If gum contour, papilla height, or crown proportions are poorly designed, the final restoration appears artificial. A restoration that functions well yet looks unnatural becomes a source of visible disappointment.
- Financial Compression: Implant therapy sometimes requires a phased treatment protocol, including bone grafting, sinus lift procedures, or provisional restorations before final crown placement. When patients expect a single-stage solution but encounter staged interventions, financial strain and timeline extension generate frustration.
- Provider Skill Variability: Implant placement demands accurate diagnostic imaging, surgical positioning, and occlusal calibration. Errors in angulation, depth, or prosthetic alignment increase the likelihood of discomfort, aesthetic imbalance, or mechanical complications. Differences in clinician expertise remain a central factor in post-treatment dissatisfaction.
Are Implant Regrets Common or Rare?
No, implant regrets are not common. Dental implant treatment demonstrates a 90–95% long-term survival rate, making it one of the most predictable procedures in restorative dentistry. In most cases, implants remain stable, functional, and biologically integrated for many years.
Importantly, the rate of regret does not parallel the complication rate. An implant can survive successfully in bone while a patient feels dissatisfied for emotional, aesthetic, or financial reasons. At the same time, minor clinical complications do not automatically result in regret when they are managed with clear communication and proper follow-up.
A significant portion of dissatisfaction stems from communication gaps rather than structural failure. When healing timelines, sensation differences, staged treatment protocols, or full cost breakdowns are not explained in detail before surgery, patients interpret normal post-operative experiences as negative outcomes.
What Problems Cause Regret Years Later?
Regret does not always appear immediately after implant placement. No, most long-term regret does not begin at surgery day. Dissatisfaction tends to follow a time-based progression, where different biological or mechanical issues surface at different stages. Segmenting complications by timeline provides clarity that standard implant discussions rarely present.
0–3 Months: Early Healing Phase:
- Early infection: Bacterial contamination during initial healing disrupts osseointegration and triggers inflammation.
- Implant mobility: Movement during integration signals failure of bone attachment and requires intervention.
Regret in this phase is linked to fear of failure and uncertainty about treatment stability.
1–3 Years: Functional Adaptation Phase:
- Peri-implantitis: Progressive inflammation around the implant leads to soft tissue damage and bone loss.
- Screw loosening: Mechanical instability of the abutment or prosthetic screw causes bite imbalance and discomfort.
Here, dissatisfaction develops when patients expect permanence yet encounter maintenance issues.
5+ Years: Long-Term Structural Changes:
- Bone remodeling: Gradual changes in bone density or contour affect tissue support around the implant.
- Crown wear: Prosthetic materials experience surface wear, chipping, or aesthetic degradation.
- Hygiene fatigue: Decline in long-term oral hygiene discipline increases inflammation risk.
Time segmentation adds information gain by demonstrating that regret is not a single event. Early-phase regret centers on integration stability, mid-term regret reflects inflammatory or mechanical concerns, and late-phase regret connects to maintenance and structural aging. Understanding this progression reframes implant dissatisfaction as a time-dependent risk pattern, not a random outcome.
Can You Remove Dental Implants If You Regret Them?
Yes. Dental implants can be removed in a controlled clinical setting. Removal follows defined surgical protocols designed to protect surrounding bone and preserve future treatment options. Transparent discussion of these methods remains limited in most implant content.
- Reverse Torque Removal: A minimally invasive technique used when implant integration is weak or moderate. The clinician applies controlled counter-rotational force to disengage the implant from bone. This method preserves more surrounding bone and reduces surgical trauma.
- Surgical Trephine Removal: Used when the implant is firmly integrated. A cylindrical trephine bur isolates the implant with a precise ring cut around it. The implant is then removed together with a thin layer of surrounding bone. This approach requires careful depth and angulation control.
- Bone Preservation Protocol: After removal, the socket is thoroughly debrided to eliminate inflamed or infected tissue. Bone graft material is placed when necessary to maintain ridge volume and structural integrity. Proper preservation supports future implant placement.
- Healing Period (3–6 Months): Bone remodeling and soft tissue stabilization occur during this phase. The site regains structural density before reassessment for further treatment.
- Re-Implantation Success (~90% with Guided Bone Regeneration): When guided bone regeneration is performed correctly, re-implantation success approaches approximately 90 percent. Systemic health, hygiene discipline, and surgical planning strongly influence this outcome.
Removal does not eliminate future options. With structured protocols and bone management, implant treatment remains reversible and reconstructable.
Do Dental Implants Feel Like Real Teeth?
No, dental implants do not feel identical to natural teeth. Although they restore strength, stability, and appearance, their biological structure differs in a fundamental way. Natural teeth are connected to the jawbone through a periodontal ligament, a microscopic connective tissue that absorbs shock and provides detailed sensory feedback. Dental implants integrate directly with bone through osseointegration and lack this ligament, creating a more rigid connection. As a result, proprioceptive feedback is reduced, meaning subtle pressure detection and fine bite sensitivity differ from natural teeth.
Despite this sensory distinction, implants provide stable chewing efficiency and strong load-bearing performance, allowing patients to eat and speak confidently. A defined adaptation phase follows placement of the final crown, during which the neuromuscular system adjusts to new bite dynamics. As adaptation progresses, awareness of the implant decreases significantly. Many articles emphasize durability and aesthetics yet avoid explaining this sensory difference, even though it plays a central role in patient expectations.
How to Avoid Regretting Dental Implants
Regret prevention begins before surgery, not after complications. A structured diagnostic and communication protocol significantly reduces dissatisfaction risk. The following checklist outlines the core pillars of predictable implant treatment.
- CBCT-Based Planning:Three-dimensional imaging with CBCT scanning ensures accurate evaluation of bone volume, density, and anatomical structures such as nerves and sinuses. Precise planning reduces angulation errors and improves long-term stability.
- Occlusal Analysis:A detailed bite assessment identifies force distribution patterns, parafunctional habits such as bruxism, and jaw alignment issues. Balanced occlusion protects the implant from overload and mechanical stress.
- Soft Tissue Evaluation: Healthy and adequate keratinized gum tissue supports long-term aesthetics and inflammation control. Tissue thickness, contour, and smile line analysis influence final visual integration.
- Medical Risk Screening: Systemic factors such as uncontrolled diabetes, smoking intensity, autoimmune conditions, and medication history influence healing response. Structured risk assessment protocols protect osseointegration success.
- Expectation Calibration: Clear discussion about healing timeline, sensory differences, staged treatment phases, and full cost structure prevents psychological dissatisfaction. Patients who understand the adaptation period report higher confidence post-treatment.
- Maintenance Commitment: Implants require long-term oral hygiene discipline and professional maintenance visits. Plaque control and periodic monitoring reduce the risk of peri-implant inflammation and late-stage bone loss.