
Porcelain veneers and Laminate Veneers differ in thickness, enamel preparation, durability, and aesthetic precision. Porcelain veneers cost €300–€850 per tooth in Turkey versus €1,000–€2,500+ in the US/UK, with a 10–15+ year lifespan and full shape correction. Laminate Veneers cost €350–€950 per tooth in Turkey versus €900–€2,000 in the US/UK, with a 5–10 year lifespan and minimal enamel reduction. The choice depends on the depth of cosmetic correction needed, long-term durability priorities, and total invested value across replacement cycles.
Patients comparing traditional porcelain veneers and ultra-thin no-prep Laminate Veneers usually evaluate four variables: aesthetic transformation depth, longevity, reversibility, and total treatment cost. The decision frame extends beyond initial price into replacement frequency, structural impact on natural enamel, and how the result integrates into a broader smile design plan.
What Are Porcelain Veneers and Laminate Veneers?
Porcelain veneers are custom-crafted ceramic shells bonded to the front surface of teeth following controlled enamel preparation, designed to correct shape, alignment, color, and proportion. Laminate Veneers are ultra-thin laminate veneers placed over existing enamel with minimal or no preparation, prioritising tooth-structure preservation over full transformation.
Porcelain veneers integrate into comprehensive aesthetic planning supported by Digital Smile Design, where each restoration is mapped to facial proportions, lip dynamics, and bite function. Laminate Veneers follow a more conservative protocol: the laminate is etched, bonded, and seated without removing meaningful tooth structure, which preserves reversibility in select cases.
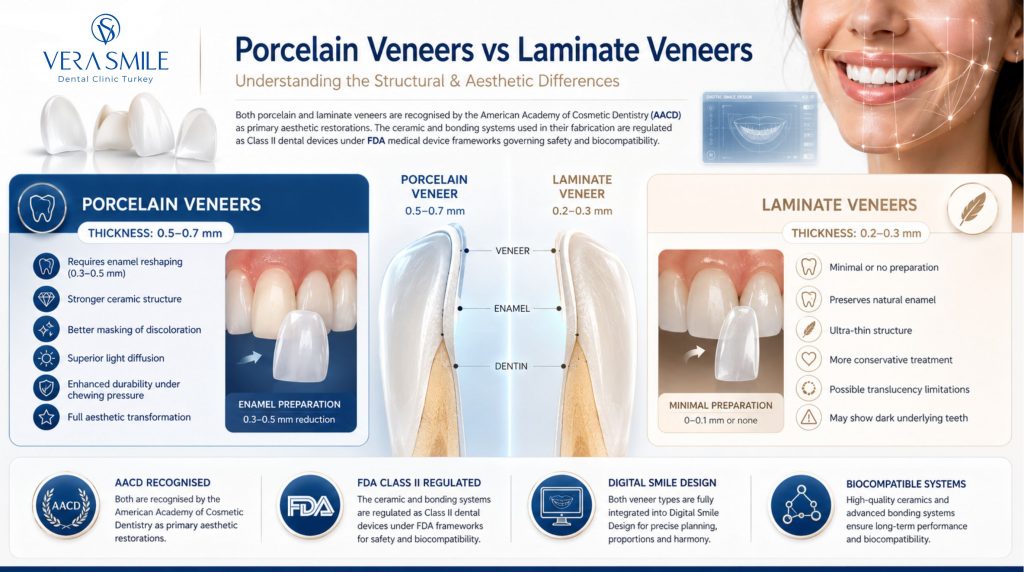
Both treatment categories are recognised by the American Academy of Cosmetic Dentistry (AACD) as primary aesthetic restorations, and the ceramic and bonding systems used in their fabrication are regulated as Class II dental devices under FDA medical device frameworks governing safety and biocompatibility.
How Do Porcelain and Laminate Veneers Differ in Structure and Thickness?
The primary structural difference lies in thickness and material strength, which directly affect durability, optical properties, and aesthetic control. Each veneer category has a defined thickness range and a corresponding preparation profile.
- Porcelain Veneers (0.5–0.7 mm): Require 0.3–0.5 mm of enamel reshaping to ensure natural fit, marginal adaptation, and accurate light reflection.
- Laminate Veneers (0.2–0.3 mm): Ultra-thin laminate shells placed over existing enamel without significant reduction.
Thicker porcelain delivers superior light diffusion, masking ability, and stress distribution under chewing load. Thinner Laminate Veneers preserve tooth structure but carry a higher chance of bulkier appearance, opacity mismatch, or visible underlying discoloration when applied over darker substrates.
Which Veneer Type Delivers Better Aesthetic Results?
Porcelain veneers deliver better aesthetic results in most clinical cases due to controlled preparation, material thickness, and advanced optical properties. Four clinical factors drive this aesthetic advantage over ultra-thin laminate alternatives.
- Controlled Tooth Preparation: Defined enamel reduction creates space for accurate contour, marginal seal, and proportionate tooth shape.
- Material Thickness: A 0.5–0.7 mm ceramic layer enables full colour masking, structural correction, and reliable stress distribution.
- Light-Reflection Properties: Higher-grade porcelain mimics natural enamel translucency, producing depth and shade accuracy that thin laminates cannot match.
- Full Smile Control: Porcelain allows calibrated correction of colour, symmetry, and proportion across the entire smile arch within a single design plan.
Ultra-thin laminate veneers cannot consistently replicate this level of aesthetic precision, which is why porcelain remains the preferred choice in moderate to severe cosmetic cases.
What Aesthetic Results Do Porcelain Veneers vs Laminate Veneers Deliver?
Porcelain veneers are designed for full aesthetic transformation where both colour and structure need correction. The table below summarises the four primary aesthetic capabilities and the clinical scope each one addresses.
| Aesthetic Property | Clinical Scope |
| High Translucency | Material thickness enables light diffusion that mimics natural enamel optical properties. |
| Deep Stain Coverage | Effective masking of tetracycline staining, fluorosis, and root canal-induced discoloration. |
| Full Reshaping | Correction of crooked, rotated, worn, or chipped teeth without orthodontic intervention. |
| Symmetry Adjustment | Calibration of tooth proportions and incisal edges across the full smile arch. |
These combined properties make porcelain the preferred ceramic in cases involving significant colour or shape correction.
How Long Do Porcelain Veneers and Laminate Veneers Last?
Porcelain veneers last significantly longer than Laminate Veneers due to stronger bonding, denser ceramic structure, and improved stress distribution. The lifespan gap directly affects total treatment cost across replacement cycles.
| Veneer Type | Average Lifespan | Material Strength | Replacement Frequency |
| Porcelain Veneers | 10–15+ years | High | Low |
| Laminate Veneers | 5–10 years | Moderate | Moderate |
Porcelain veneers resist fracture, chipping, and surface wear in published clinical follow-up data, while ultra-thin laminate veneers show higher rates of debonding, marginal staining, and aesthetic deterioration over time. Patients prioritising long-term value across a single treatment cycle gravitate toward porcelain in most clinical decisions.
Systematic reviews of porcelain laminate veneer survival report a 10-year clinical success rate of 91–95% when bonding occurs on intact enamel, and retrospective evaluations following cases over 7–14 years confirm durability at the upper end of the published lifespan range.
Is Tooth Preparation Required for Both Veneer Types?
No. Tooth preparation is required for porcelain veneers but not for laminate veneers. Preparation is a controlled clinical step that improves marginal fit, bonding strength, and long-term stability, rather than a disadvantage.
How Much Tooth Preparation Do Porcelain vs Laminate Veneers Require?
Porcelain veneers require 0.3–0.7 mm of controlled enamel reduction, while laminate veneers require no or minimal enamel removal. The difference reflects two distinct clinical philosophies: porcelain prioritises aesthetic transformation and long-term marginal stability through defined preparation, whereas laminate veneers prioritise preservation of natural tooth structure through a conservative bonding protocol.
In porcelain cases, enamel reduction is planned according to the desired aesthetic outcome and the starting tooth position. The 0.3–0.7 mm removal creates the space needed for accurate fit, contour, and light reflection, and allows correction of moderate alignment issues without orthodontic treatment. Once performed, the reduction is irreversible and requires permanent restorative cover, which is why the preparation profile defines the long-term clinical behaviour of the restoration.
Laminate veneers follow the opposite logic. Placement involves no or minimal reduction during bonding, which keeps the enamel surface largely intact and preserves reversibility in select cases where the bonding has not modified the tooth. This conservative scope limits adaptability to moderate or complex aesthetic corrections, since the underlying tooth shape, alignment, and shade remain visible through the thin laminate layer.
Preparation directly affects final aesthetics, marginal seal, and longevity. The choice between the two approaches is a controlled clinical step driven by case complexity, not a disadvantage of either method. Veneers bonded to intact enamel show significantly lower long-term failure rates compared to veneers bonded to exposed dentin, directly influencing durability and clinical success, according to the Journal of Prosthetic Dentistry.
How Much Do Porcelain Veneers and Laminate Veneers Cost in Turkey vs the US and UK?
Porcelain veneers cost more than Laminate Veneers in most markets due to laboratory craftsmanship, ceramic material grade, and the precision required during preparation. Pricing in Turkey is 60–75% lower than in the United States and United Kingdom for clinically equivalent treatment.
| Veneer Type | Cost per Tooth (Turkey) | Cost per Tooth (US/UK) | Included Scope |
| Porcelain Veneers | €300 – €850 | €1,000 – €2,500+ | Design, prep, lab fabrication, fitting |
| Laminate Veneers | €350 – €950 | €900 – €2,000 | Minimal prep, placement |
| Full smile (10–20 veneers) | €3,000 – €14,000 (Turkey) | €10,000 – €40,000+ (US/UK) | Smile design, prep, lab, placement |
For a comprehensive cost reference, see dental veneers cost. Patients researching dental veneers in Turkey prioritise total invested value across replacement cycles rather than the initial quote, since lifespan directly affects total spend per decade.
What Affects the Cost of Porcelain and Laminate Veneers?
Veneer pricing is driven by material selection, preparation depth, lab fabrication standards, and the scope of smile design integrated into the treatment plan. Understanding these drivers allows patients to compare quotes across providers and identify which components are negotiable versus fixed.
- Material grade: Feldspathic, lithium disilicate (e.max), and zirconia-reinforced porcelain carry different cost tiers, with lithium disilicate the most common premium ceramic for full smile cases.
- Number of veneers placed: Single-tooth placements carry a higher per-unit cost than full-arch smile design, since fixed lab and chairside overhead is distributed across more units in larger cases.
- Smile design protocol: Cases planned with Digital Smile Design require additional imaging, mock-up, and provisional fabrication, raising per-tooth cost while improving predictability.
- Tooth condition: Pre-existing decay, fracture lines, or worn enamel demand restoration or build-up before veneer placement, adding cost outside the standard scope.
- Provider experience: Specialist prosthodontists and aesthetic dentists with documented case portfolios charge a premium that correlates with lower revision rates.
- Lab partnership: Domestic ceramist labs with accredited workflow control deliver superior optical results and adhesion outcomes versus generic offshore labs.
- Geographic market: Premium urban markets in the US (NYC, LA, SF) and UK (London) routinely charge 40–80% above national averages for the identical CDT procedure code.
These factors compound across a full smile case, which is why quote ranges from different providers can vary by several thousand euros for clinically similar treatment plans.
What Are the Hidden Costs Patients Routinely Miss in Veneer Treatment Plans?
Published per-tooth quotes consistently exclude ancillary charges that appear on the final invoice. Budget accurately by accounting for the following components.
| Hidden Cost Item | Approximate US Range | Notes |
| Diagnostic imaging (panoramic + intraoral) | €75 – €250 | Required for planning; rarely included in headline quote |
| Smile design mock-up / wax-up | €150 – €600 | Often a separate fee outside per-tooth pricing |
| Temporary veneers (provisionals) | €50 – €150 per tooth | In-office or lab-fabricated; standard for prep cases |
| Bite adjustment / occlusal refinement | €100 – €300 | Post-cementation occlusion calibration |
| Replacement after fracture or debonding | €900 – €2,500+ per tooth | Single-unit replacement of one veneer |
| Night guard (post-treatment protection) | €150 – €700 | Strongly indicated for bruxism patients |
| Maintenance polishing visits | €80 – €200 per visit | Recommended every 6–12 months |
Patients combining veneer treatment with composite bonding on adjacent teeth, teeth whitening on non-restored teeth, or dental crowns on heavily damaged molars consolidate procedures into a single treatment phase, which removes incremental imaging, lab, and visit fees.
How Long Is the Recovery and Adjustment Period After Veneer Placement?
The recovery curve after veneer placement is short compared with most aesthetic dental procedures. Patients return to standard activities within 24 hours, and the gum and bite adjustment phase extends across 7–14 days through five defined stages.
- Day 0 (Placement): Mild gingival pressure and transient cold sensitivity are expected, with a soft diet for 24 hours, avoidance of pigmented foods such as coffee and red wine, and contact required for persistent sharp pain or any veneer mobility.
- Days 1–3: Settling sensitivity and gum adaptation to new margins continue, with gradual reintroduction of normal foods and warm saline rinses 2–3 times daily, while marginal pain at a single veneer, a visible chip, or persistent gum bleeding requires contact.
- Days 4–7: Sensitivity resolves and the bite stabilises as gum contour normalises, with routine flossing and standard brushing resumed at the margins, while new or intensifying cold sensitivity or a loose veneer warrants contact.
- Days 8–14: Near-complete adaptation occurs with normal speech and a settled aesthetic result, with an occlusal check-up scheduled around week 2, while continued sensitivity beyond day 14 or a visible margin opening requires clinical review.
- 4–6 Weeks: Full functional integration is achieved with no daily awareness of the veneers, full oral hygiene is resumed and a night guard is considered in bruxism cases, while recurrent sensitivity or visible gum recession at the margin signals the need for follow-up.
The most common adjustment issue is occlusal interference at one or two veneers, resolved with a 5-minute polish appointment. Long-term protection is driven by night guard wear in bruxism patients and biannual maintenance polishing.
Are Porcelain or Laminate Veneers Better for a Smile Makeover?
Yes. Porcelain veneers are better for a full smile makeover. They provide the adaptability, optical performance, and structural control required for complete aesthetic transformation within a comprehensive treatment plan.
A structured smile makeover involves several integrated planning steps that determine the final aesthetic and functional outcome.
- Facial analysis: Assessment of lip dynamics, midline alignment, and facial proportion in motion.
- Tooth proportion planning: Calibration of width-to-length ratios according to golden ratio standards.
- Shade matching: Coordinated colour selection across the visible smile arch.
- Functional alignment: Bite calibration and occlusal adjustment integrated into the design.
- Gingival contouring: Correction of uneven gum lines that compromise smile symmetry.
Laminate Veneers lack the structural and optical flexibility required for full-arch transformation, which restricts their role in advanced aesthetic dentistry. Patients pursuing comprehensive treatment in Turkey routinely combine porcelain veneers with adjunct procedures within a single visit, including Hollywood Smile in Turkey protocols that integrate gingival aesthetics, whitening of non-restored teeth, and bite refinement.
Why Do International Patients Choose Turkey for Veneer Treatments?
Due to cost efficiency, clinical standards, and coordinated treatment pathways designed for medical travel, international patients choose to have their dental treatments in Turkey. The combination of these factors makes Turkey one of the most accessed destinations for aesthetic dentistry.
- Cost Advantage: 60–75% lower pricing compared to the US and UK for equivalent veneer treatments.
- Clinical Standards: Internationally accredited clinics using Digital Smile Design, CAD/CAM systems, and modern ceramic materials.
- All-Inclusive Packages: Transparent pricing covering consultation, planning, fabrication, placement, and follow-up.
- Treatment Efficiency: Complete smile transformations delivered within 5–10 days.
- Integrated Care: Combination of veneers with teeth whitening, gingival contouring, and smile makeover protocols.
- Medical Travel Support: VIP transfers, hotel accommodation, and multilingual patient coordination.
This structure allows international patients to access aesthetic dentistry with consistent clinical standards and reduced total treatment cost.
Which Veneer Type Suits Complex Cosmetic Cases?
Porcelain veneers are the preferred solution for moderate to severe cosmetic and structural concerns. Laminate Veneers serve a narrow indication range focused on minor enhancements.
Which Cases Indicate Porcelain Veneers?
Porcelain veneers are indicated when both aesthetic and structural correction are required. The clinical indication range covers a defined set of moderate to severe cosmetic concerns.
- Crooked or rotated teeth: Visual alignment correction without orthodontic treatment.
- Severe discoloration: Tetracycline staining, fluorosis, or root canal-induced darkening.
- Worn or chipped edges: Reconstruction of uneven incisal edges and aesthetic asymmetry.
- Microdontia: Reshaping of proportionally small teeth to restore arch balance.
- Full smile makeover: Cases requiring integrated bite alignment and smile design planning.
These indications cover the majority of clinical scenarios where comprehensive aesthetic transformation is the patient goal.
Which Cases Indicate Laminate Veneers?
Laminate veneers are suitable only when minimal intervention is sufficient. The indication range is limited to surface-level enhancements on intact teeth.
- Minor diastemas: Small gaps under 1 mm in width.
- Slight colour enhancement: Shade refinement on already-light teeth.
- Reversibility priority: Patients hesitant about enamel reduction or committed to a conservative approach.
- Single-tooth refinement: Shape adjustment on aesthetically sound teeth without alignment issues.
Patients evaluating veneers for moderate misalignment benefit from comparing options through bonding vs veneers, particularly when conservative reshaping is sufficient and reversibility matters.
Which Veneer Type Do Dentists Recommend for Long-Term Results?
Dentists recommend porcelain veneers for predictable, long-term aesthetic outcomes in most cases. The clinical preference is driven by documented survival data and superior performance under chewing load.
- Adhesive interface: Stronger bonding to prepared enamel compared with no-prep laminate placement.
- Stress distribution: Improved load handling during chewing and parafunction.
- Patient satisfaction: Higher reported satisfaction in full-arch and full-mouth cases.
- Revision rates: Lower revision rates documented across 10-year clinical follow-up studies.
Laminate Veneers remain suitable for select patients with minimal cosmetic needs, reversibility priorities, or specific budget structures, but they appear in a narrow segment of complex smile rehabilitation cases.
Narrative literature reviews of clinical survival rates and laboratory failure mechanisms across the dental veneer category support porcelain as the long-term standard for predictable outcomes. The Cleveland Clinic and NHS cosmetic dentistry guidelines reference porcelain veneers as the standard restorative approach for moderate-to-severe aesthetic indications.
FAQ’s
When Should Patients Choose Alternatives to Veneers?
Patients should choose alternatives to veneers when the tooth structure, bite dynamics, or treatment goals exceed what veneers are designed to correct. Veneers are surface restorations, and forcing them into structurally or functionally complex cases leads to compromised results and higher failure risk.
When Are Dental Crowns More Appropriate Than Veneers?
Dental crowns are more appropriate than veneers when the remaining tooth structure cannot reliably support a veneer bond. This applies to teeth that are heavily restored with limited intact enamel, anterior teeth that have undergone root canal treatment and show structural compromise, and cases involving severe parafunction such as heavy bruxism or clenching, where full coverage is required to protect the underlying tooth from fracture and long-term failure.
When Is Composite Bonding the Better Choice?
Composite bonding is the better choice when aesthetic correction is minor and preservation of natural tooth structure is the priority. It is well suited for single-tooth chips or small defects, particularly in younger patients, as it requires minimal or no enamel removal. It fits cases where budget constraints influence treatment selection and reversibility is important, and it is frequently used as a diagnostic or transitional phase before committing to definitive ceramic restorations.
When Should Orthodontic Treatment Come First?
Orthodontic treatment should come first when tooth alignment and bite cannot be corrected with surface restorations alone. This includes cases with moderate to severe crowding or rotation, Class II or Class III bite discrepancies, and functional occlusion issues that affect long-term stability. It is necessary when achieving alignment with veneers would require excessive enamel removal, compromising tooth integrity.