
There is no upper age limit for dental veneers. Candidacy depends on gum health, bone support, enamel coverage, salivary flow, and medical status, not on chronological age, and patients in their 60s, 70s, and 80s receive veneers routinely when the supporting tissues are healthy. Age-related factors such as gum recession, dry mouth from medications, root sensitivity, bruxism, and existing crowns or fillings do not rule out veneers, but they shift material choice and timing. Lithium disilicate (E.max) and no-prep porcelain are recommended most in this age group because they conserve enamel, and veneers here can last 10 to 20 years under stable periodontal conditions. Where veneers do not fit, composite bonding, crowns, partial-coverage ceramics, or whitening are matched to the case after assessment.
Is There an Age Limit for Dental Veneers?
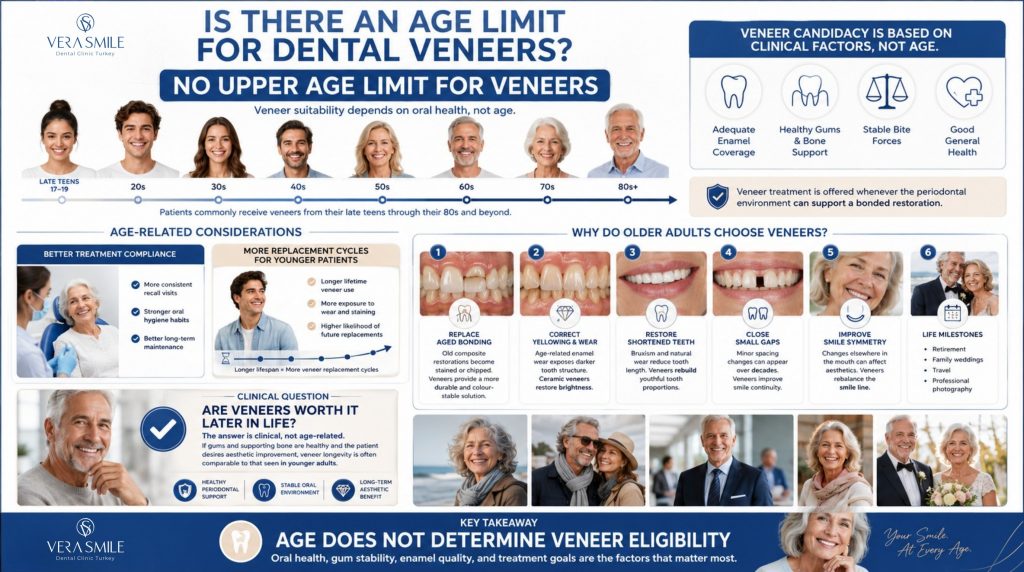
No. There is no upper age limit for dental veneers. Veneer candidacy is decided by clinical variables that are independent of age, including enamel coverage at the planned margin, gum and bone stability, occlusal load, and general medical status.
Two age-related patterns appear in practice. Older adults often show more consistent recall attendance and stricter oral hygiene than younger cohorts, while younger patients accumulate more replacement cycles because their total lifetime exposure to wear, staining, and bonding fatigue is longer. Treatment is offered whenever the periodontal environment can support a bonded restoration. The youngest patients receiving veneers are usually in their late teens after permanent tooth development is complete, while the oldest have included individuals in their 80s and beyond.
Why Do Older Adults Choose Veneers?
Older adults choose veneers for the same reasons younger patients do, with three additional age-specific drivers: replacement of aged direct composites, correction of darkened or worn front teeth, and restoration of confidence after retirement or major life events.
Common reasons in this age group include:
- Aged bonding replacement: Discoloured or chipped composite bonding placed 10 to 15 years earlier is replaced with a shade-stable restoration.
- Enamel wear and yellowing: Surface wear and intrinsic yellowing that intensify with age are masked by ceramic.
- Shortened front teeth: Long-term attrition or bruxism reduces incisal length, which veneers restore.
- Small gaps: Spaces that appear as tissues remodel over decades are closed.
- Smile-line symmetry: Tooth loss elsewhere that has changed the smile line is rebalanced.
- Milestone events: Retirement portraits, family weddings, or extended travel prompt aesthetic updates.
Clinical note: Many older patients ask whether veneers are worth it later in life. The answer is clinical, not philosophical. If the gums and bone are healthy and the patient values the aesthetic change, lifespan in this age group commonly matches that of younger adults.
Are Veneers Safe for Older Adults?
Yes. Dental veneers are safe for older adults when periodontal status, salivary flow, and general medical condition support the procedure. Local anaesthesia is well tolerated in older adults under routine medical management, and the procedure itself is identical for older and younger patients.
The age-specific safety considerations sit in the medical history rather than the procedure. Most veneer work involves little bleeding, so cardiac and antiplatelet medications are rarely a barrier, and the dental team coordinates with the prescribing physician when needed. Controlled diabetes does not contraindicate veneers, though uncontrolled diabetes raises gum and bone risk and should be stabilised first. Because veneers do not expose jaw bone, bisphosphonate-related osteonecrosis risk is not relevant to standard placement, and bleeding disorders are managed with modern low-trauma preparation plus a medical review where indicated. Cognitive status matters only in that patients must be able to attend multiple visits and follow aftercare, so treatment is paced accordingly. The pre-treatment medical review is the single additional safety step.
Which Dental Conditions in Older Adults Affect Veneer Treatment?
Several age-related dental conditions affect veneer candidacy and material choice, including gum recession, xerostomia, root sensitivity, bruxism, attrition, and existing extensive restorations. Each condition has a defined clinical management step.
- Gum recession: Receded margins expose root surfaces that do not bond to porcelain as reliably as enamel, so margins are adjusted or the case is staged after periodontal stabilisation.
- Xerostomia (dry mouth): Common with antihypertensives, antidepressants, or diuretics, reduced saliva raises caries risk at the margin, so preventive fluoride and saliva-substitute protocols are added.
- Root sensitivity: Exposed dentine on the cervical third of older teeth may require desensitising treatment before preparation.
- Bruxism and attrition: Long-standing grinding reduces tooth height and may indicate a stronger material such as lithium disilicate or zirconia, plus a custom night guard.
- Periodontal disease history: Stable, treated periodontal disease is compatible with veneers, while active disease must be controlled before treatment begins.
Patient tip: A pre-treatment periodontal assessment is the most important step for older patients considering veneers. Bone and gum stability decides whether veneers are placed now, after periodontal therapy, or replaced by another option entirely.
Can Veneers Be Placed on Teeth with Crowns or Fillings?
No, a veneer cannot be placed on a tooth that already has a crown, because no enamel surface remains to bond to, so the crown is replaced with a new crown or another aesthetic restoration instead. A tooth with a filling is judged by how much enamel is left.
A small composite filling usually leaves enough enamel for a veneer, and the existing composite is partially included in the preparation. A large composite filling is workable only when at least 50% of the bonding surface remains enamel; below that, a crown is more predictable. A tooth treated with a previous root canal can take a veneer if enough sound structure remains and there is no sign of fracture, though a crown or onlay is often the safer choice. An old porcelain veneer is removed and replaced rather than bonded over, because adhesion to aged cement is unreliable. A digital scan and intraoral examination quickly identify which teeth in an older patient’s smile are veneer-suitable and which need an alternative restoration, such as dental crowns.
How Long Do Veneers Last in Older Patients?
Dental veneers in older patients last between 10 and 20 years, similar to younger adults, when periodontal conditions are stable and the patient maintains regular hygiene visits. Lithium disilicate and porcelain veneers carry the strongest long-term survival evidence.
Three factors set the lifespan in this age group, and the first outweighs the others. Bone and gum stability is decisive, since active recession or alveolar bone loss is the most common cause of late-stage veneer compromise in older patients; a veneer placed on a stable foundation in an 80-year-old can outlast one placed on a younger patient with untreated recession. Hygiene consistency comes next, and patients with reduced manual dexterity benefit from electric brushes and interdental aids. Bite control is the third factor, because bruxism accumulated over years shortens lifespan unless a night guard is worn. Lifespan is therefore governed by tissue condition and maintenance discipline rather than age, and a six-month recall that monitors margins and bite is what carries a restoration to the upper end of the 10 to 20 year range.
What Are the Alternatives to Veneers for Older Adults?
Alternatives to veneers for older adults include composite bonding, full-coverage crowns, partial-coverage ceramics, professional whitening, and full-arch rehabilitation, each preferred in a specific clinical situation.
- Composite bonding: Best for a single tooth or minor correction and for sensitive cases; it lasts 5 to 7 years and is mostly reversible.
- Full-coverage crown: Best for teeth with large fillings, root canal treatment, or significant structural loss; it lasts 10 to 20 years and is not reversible.
- Partial-coverage ceramic (onlay): Best for teeth with structural loss but an intact front surface; it lasts 10 to 15 years and is not reversible.
- Professional whitening: Best for shade-only correction on healthy enamel; results hold 1 to 3 years between touch-ups and the option is fully reversible.
- Implant-supported restoration: Best for missing teeth in the smile zone; the implant lasts 20 years or more and the result is not reversible.
- Full-arch rehabilitation (All-on-4 / All-on-6): Best for multiple missing teeth, advanced wear, or a failing dentition; it lasts 15 to 25 years and is not reversible.
Many older patients benefit from a combined plan: veneers on healthy front teeth, dental crowns on heavily restored teeth, and teeth whitening on adjacent natural teeth to match the new shade. Where the whole dentition is failing, full mouth dental implants may be the more durable route.
What Is the Veneers Procedure Like for Older Patients?
The veneers procedure for older patients follows the same clinical workflow as for any adult, with three age-relevant adaptations: longer rest periods between stages, modified medication scheduling, and customised hygiene preparation.
Adaptations commonly used include:
- Shorter appointment blocks: Stages are split to accommodate posture comfort.
- Saliva control: Absorbent aids are used when xerostomia is significant.
- Desensitising pre-treatment: Sensitive exposed dentine is treated before preparation.
- Soft-tissue management: Thin or receded gums are managed before bonding.
- Coordinated medication timing: Anticoagulants and antihypertensives are scheduled with the prescribing physician.
Anaesthesia is the same as for younger adults, and the recovery experience is similar.
How Should Older Patients Care for Veneers?
Older patients should care for veneers with the same daily routine as younger adults, with extra attention to gum margins, saliva flow, and bite control. The daily and routine maintenance items are summarised below.
- Brush twice daily: Use a soft-bristled or electric brush to clean the margin gently without abrading the glaze.
- Low-abrasive toothpaste: Avoid surface wear on porcelain or composite.
- Floss or interdental brushes: Clean the gum line daily, where recurrent caries is most likely in this age group.
- Manage dry mouth: Stay hydrated and consider saliva substitutes, since reduced saliva raises caries risk at the margin.
- Six-month cleanings: Attend professional recall for bite checks and margin assessment.
- Night guard: Wear a guard if bruxism is identified, regardless of age.
- Avoid tooth misuse: Do not use teeth to open packaging or bite hard items.
- Quit smoking: Tobacco discolours cement and accelerates recession.
Patient tip: Older patients with arthritis or reduced grip can use wide-handled toothbrushes and electric brushes with timer modes to maintain effective plaque removal. A dental hygienist can demonstrate adapted technique during the recall visit.
Patients who grind heavily can ask about a custom mouth guard for grinding teeth to protect the restorations overnight.
Which Type of Veneer Is Most Suitable for Older Adults?
Lithium disilicate (E.max) and no-prep porcelain veneers are the materials most commonly recommended for older adults because they preserve enamel, accommodate sensitive teeth, and deliver long-term durability. Feldspathic porcelain remains a strong choice for maximum natural translucency, and composite is reserved for cases where reversibility or budget is the priority.
- Lithium disilicate (E.max): Best all-round option for older adults, combining strength, thin preparation, and 12 to 20 years of expected service.
- No-prep porcelain (including Lumineers): Ideal for sensitive teeth and patients who want minimal intervention, as covered under Lumineers.
- Feldspathic porcelain: Highest natural translucency, best for patients prioritising aesthetics in the anterior smile zone.
- Zirconia: Reserved for older patients with heavy bruxism or significant occlusal wear.
- Composite: Suitable for single-tooth correction, budget cases, or as a reversible trial before committing to ceramic.
Patients weighing material against tooth structure can compare options through bonding vs veneers and veneers vs crowns before deciding.
Why Choose Vera Smile for Veneers in Older Adults?
Vera Smile is an Istanbul dental clinic that treats veneer cases at every adult age, planning each one around periodontal stability, conservative preparation, and materials suited to age-related conditions. Older patients choose the clinic because it combines:
- Regulatory oversight: Turkish Ministry of Health authorisation provides full regulatory oversight.
- Slow Dentistry standards: Slow Dentistry Global Network protocols mandate proper isolation, time-controlled bonding, and disinfection that protect veneer longevity.
- AACD-aligned expertise: Cosmetic protocols deliver natural shade and shape outcomes that fit mature smiles.
- Digital Smile Design: Conservative anterior planning suited to enamel-limited teeth is integrated into every full-arch case.
- CAD/CAM precision: 3D intraoral scanning and CAD/CAM dentistry deliver marginal accuracy in the 20 to 50 micron range.
- Transparent planning: Written timelines, material disclosures, and replacement projections are agreed in advance.
- International patient care: VIP airport transfers, accommodation, and remote aftercare support are tailored to travel comfort.
- Periodontal screening: Gum and bone status is verified before veneer planning, rather than assumed.
Two steps decide an older patient’s plan before any tooth is touched. Digital Smile Design previews tooth length, shape, and shade so worn edges and receded gums are accounted for and the proportions suit a mature face. The veneers cost is fixed at the same stage, since the figure shifts when a heavily filled tooth needs a crown instead, which lets the plan be budgeted in Turkey pricing before travel.
FAQ
Yes, if periodontal conditions are stable and the patient values the aesthetic change. Lifespan in this age group commonly matches younger adults when gum and bone support are healthy, so clinical rather than chronological factors decide the answer.
Yes. Veneers cover the front surface of the tooth with a shade-stable ceramic and mask intrinsic yellowing that does not respond to whitening. Composite veneers offer a less expensive route but fade faster than ceramic.
Yes, if the dentures replace teeth other than those receiving veneers and the remaining natural teeth supporting the smile have sufficient enamel and stable gums. The denture shade is coordinated with the new veneer shade so the final smile remains harmonious.
Some mild cold or air sensitivity may occur for one to two weeks after the procedure and usually resolves. Persistent sensitivity is uncommon and warrants clinical review. Older patients with pre-existing dentine exposure may receive a desensitising protocol before preparation.
No, in most countries veneers are considered cosmetic and are not covered by general health insurance. Some dental plans cover a portion when the procedure addresses functional issues such as fractured teeth, but coverage rules differ widely, so direct confirmation with the insurer is the only reliable answer.
Limited same-day combinations are possible, such as professional cleaning before veneer try-in, but veneers themselves require multiple appointments. Treatments such as periodontal therapy or extractions are completed and healed before veneer planning begins.